

Growth of lung parenchyma in infants and toddlers with chronic lung disease of infancy
- PMID: 20133928
- PMCID: PMC2874450
- DOI: 10.1164/rccm.200908-1190OC
Growth of lung parenchyma in infants and toddlers with chronic lung disease of infancy
Abstract
Rationale: The clinical pathology describing infants with chronic lung disease of infancy (CLDI) has been limited and obtained primarily from infants with severe lung disease, who either died or required lung biopsy. As lung tissue from clinically stable outpatients is not available, physiological measurements offer the potential to increase our understanding of the pulmonary pathophysiology of this disease.
Objectives: We hypothesized that if premature birth and the development of CLDI result in disruption of alveolar development, then infants and toddlers with CLDI would have a lower pulmonary diffusing capacity relative to their alveolar volume compared with full-term control subjects.
Methods: We measured pulmonary diffusing capacity and alveolar volume, using a single breath-hold maneuver at elevated lung volume. Subjects with chronic lung disease of infancy (23-29 wk of gestation; n = 39) were compared with full-term control subjects (n = 61) at corrected ages of 11.6 (4.8-17.0) and 13.6 (3.2-33) months, respectively.
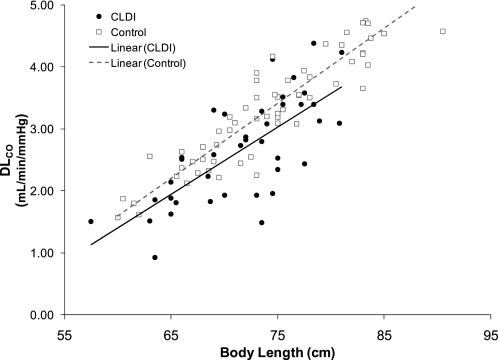
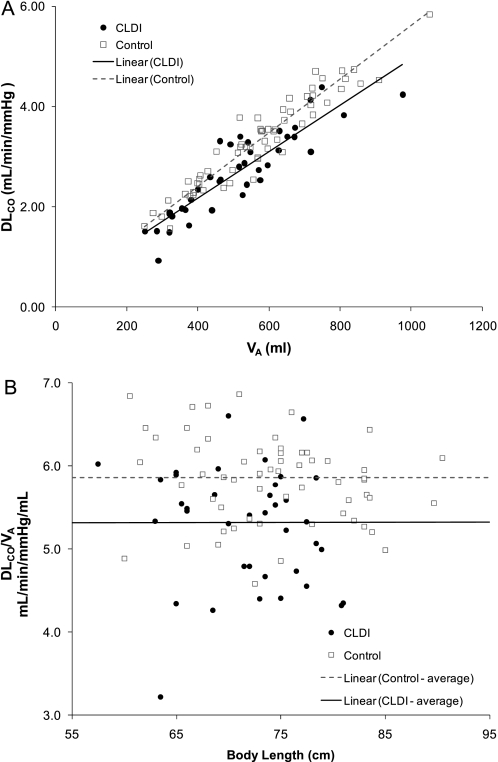
Measurements and main results: Alveolar volume and pulmonary diffusing capacity increased with increasing body length for both groups. After adjusting for body length, subjects with CLDI had significantly lower pulmonary diffusing capacity (2.88 vs. 3.23 ml/min/mm Hg; P = 0.0004), but no difference in volume (545 vs. 555 ml; P = 0.58).
Conclusions: Infants and toddlers with CLDI have decreased pulmonary diffusing capacity, but normal alveolar volume. These physiological findings are consistent with the morphometric data obtained from subjects with severe lung disease, which suggests an impairment of alveolar development after very premature birth.
Figures

References
-
- Baraldi E, Filippone M. Chronic lung disease after premature birth. N Engl J Med 2007;357:1946–1955. - PubMed
-
- Northway WH Jr, Rosan RC, Porter DY. Pulmonary disease following respirator therapy of hyaline-membrane disease. N Engl J Med 1967;267:357–368. - PubMed
-
- Jobe AJ. The new BPD: an arrest of lung development. Pediatr Res 1999;46:641–643. - PubMed
-
- Coalson JJ. Pathology of new bronchopulmonary dysplasia. Semin Neonatol 2003;8:73–81. - PubMed
-
- Husain AN, Siddiqui NH, Stocker JT. Pathology of arrested acinar development in postsurfactant bronchopulmonary dysplasia. Hum Pathol 1998;29:710–717. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
