

Endoscopic ultrasound-guided celiac plexus neurolysis using a reverse phase polymer
- PMID: 20135721
- PMCID: PMC2817061
- DOI: 10.3748/wjg.v16.i6.728
Endoscopic ultrasound-guided celiac plexus neurolysis using a reverse phase polymer
Abstract
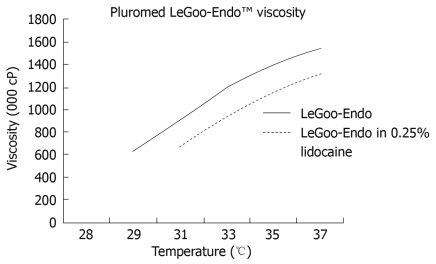
Aim: To assess the feasibility of endoscopic ultrasound (EUS)-guided celiac plexus neurolysis (CPN) using a poloxamer.
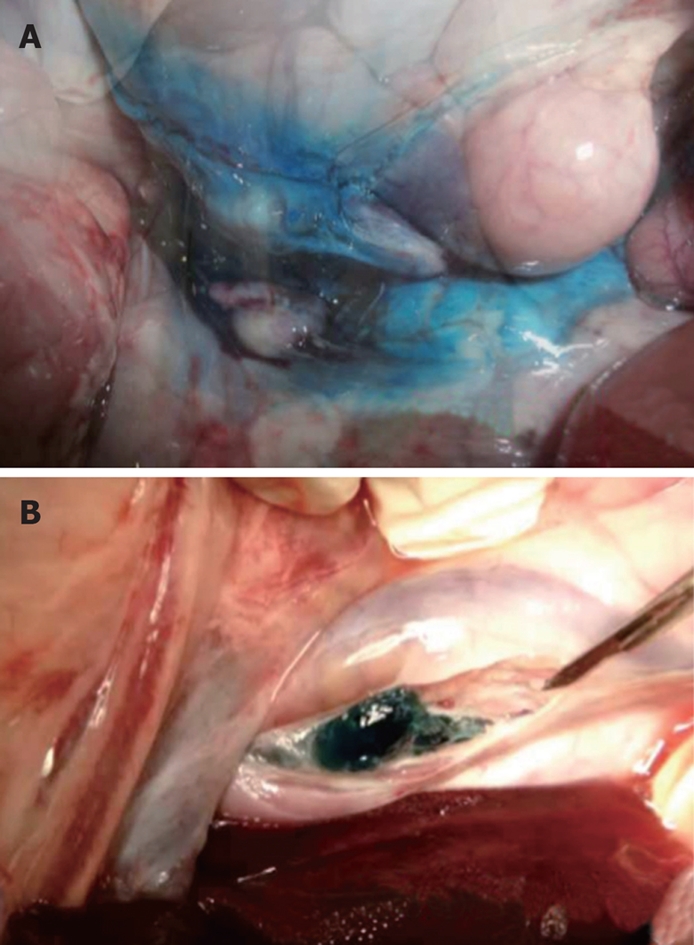
Methods: In this prospective evaluation, six Yorkshire pigs underwent EUS-guided CPN. Three received an injection of 10 mL of 0.25% Lidocaine plus methylene blue (group 1) and three received an injection of 10 mL of 0.25% Lidocaine plus blue colored poloxamer (PS137-25) (group 2). Necropsy was performed immediately after the animals were sacrificed. The abdominal and pelvic cavities were examined for the presence of methylene blue and the blue colored poloxamer.
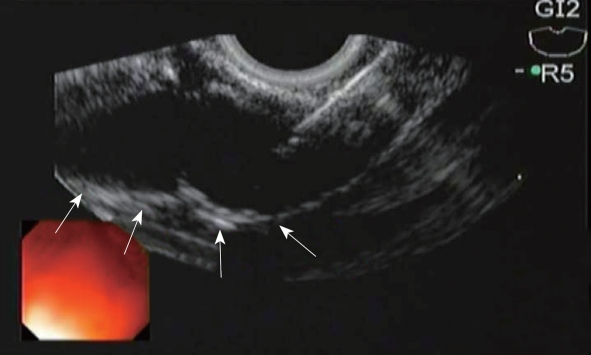
Results: EUS-guided CPN was successfully performed in all 6 pigs without immediate complication. Methylene blue was identified throughout the peritoneal and retroperitoneal cavity in group 1. The blue colored poloxamer was found in the retroperitoneal cavity immediately adjacent to the aorta, in the exact location of the celiac plexus in group 2.
Conclusion: EUS-guided CPN using a reverse phase polymer in a non-survival porcine model was technically feasible. The presence of a poloxamer gel at the site of the celiac plexus at necropsy indicates a precise delivery of the neurolytic agent.
Figures

Similar articles
-
Endoscopic ultrasound-guided celiac plexus block and neurolysis.Dig Endosc. 2017 May;29(4):455-462. doi: 10.1111/den.12824. Epub 2017 Mar 9. Dig Endosc. 2017. PMID: 28160344 Review.
-
Contrast-enhanced ultrasound-guided celiac plexus neurolysis in patients with upper abdominal cancer pain: initial experience.Eur Radiol. 2020 Aug;30(8):4514-4523. doi: 10.1007/s00330-020-06705-z. Epub 2020 Mar 24. Eur Radiol. 2020. PMID: 32211966
-
Endoscopic ultrasound-guided celiac plexus neurolysis improves pain in gallbladder cancer.Indian J Gastroenterol. 2020 Apr;39(2):171-175. doi: 10.1007/s12664-019-01003-z. Epub 2020 Feb 17. Indian J Gastroenterol. 2020. PMID: 32065352
-
A prospective, randomized study of EUS-guided celiac plexus neurolysis for pancreatic cancer: one injection or two?Gastrointest Endosc. 2011 Dec;74(6):1300-7. doi: 10.1016/j.gie.2011.07.073. Epub 2011 Oct 13. Gastrointest Endosc. 2011. PMID: 22000795 Clinical Trial.
-
Bilateral vs. unilateral endoscopic ultrasound-guided celiac plexus neurolysis for abdominal pain management in patients with pancreatic malignancy: a systematic review and meta-analysis.Support Care Cancer. 2018 Feb;26(2):353-359. doi: 10.1007/s00520-017-3888-0. Epub 2017 Sep 27. Support Care Cancer. 2018. PMID: 28956176
Cited by
-
Utility of interventional endoscopic ultrasound in pancreatic cancer.Front Oncol. 2023 Sep 15;13:1252824. doi: 10.3389/fonc.2023.1252824. eCollection 2023. Front Oncol. 2023. PMID: 37781196 Free PMC article. Review.
-
Percutaneous Fluoroscopic-Guided Celiac Plexus Approach: Results in a Pig Cadaveric Model.Animals (Basel). 2024 May 16;14(10):1478. doi: 10.3390/ani14101478. Animals (Basel). 2024. PMID: 38791695 Free PMC article.
-
Percutaneous Ultrasound Guided Celiac Plexus Approach: Results in a Pig Cadaveric Model.Animals (Basel). 2024 Dec 2;14(23):3482. doi: 10.3390/ani14233482. Animals (Basel). 2024. PMID: 39682447 Free PMC article.
-
How to improve the efficacy of endoscopic ultrasound-guided celiac plexus neurolysis in pain management in patients with pancreatic cancer: analysis in a single center.Surg Laparosc Endosc Percutan Tech. 2014 Feb;24(1):31-5. doi: 10.1097/SLE.0000000000000032. Surg Laparosc Endosc Percutan Tech. 2014. PMID: 24487155 Free PMC article.
-
Alleviating Pancreatic Cancer-Associated Pain Using Endoscopic Ultrasound-Guided Neurolysis.Cancers (Basel). 2018 Feb 15;10(2):50. doi: 10.3390/cancers10020050. Cancers (Basel). 2018. PMID: 29462851 Free PMC article. Review.
References
-
- Ventafridda GV, Caraceni AT, Sbanotto AM, Barletta L, De Conno F. Pain treatment in cancer of the pancreas. Eur J Surg Oncol. 1990;16:1–6. - PubMed
-
- Lankisch PG. Natural course of chronic pancreatitis. Pancreatology. 2001;1:3–14. - PubMed
-
- Levy MJ, Topazian MD, Wiersema MJ, Clain JE, Rajan E, Wang KK, de la Mora JG, Gleeson FC, Pearson RK, Pelaez MC, et al. Initial evaluation of the efficacy and safety of endoscopic ultrasound-guided direct Ganglia neurolysis and block. Am J Gastroenterol. 2008;103:98–103. - PubMed
-
- Tran QN, Urayama S, Meyers FJ. Endoscopic ultrasound-guided celiac plexus neurolysis for pancreatic cancer pain: a single-institution experience and review of the literature. J Support Oncol. 2006;4:460–462, 464; discussion 463-464. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
