

Out-of-hospital endotracheal intubation experience and patient outcomes
- PMID: 20138400
- PMCID: PMC3071147
- DOI: 10.1016/j.annemergmed.2009.12.020
Out-of-hospital endotracheal intubation experience and patient outcomes
Abstract
Study objective: Previous studies suggest improved patient outcomes for providers who perform high volumes of complex medical procedures. Out-of-hospital tracheal intubation is a difficult procedure. We seek to determine the association between rescuer procedural experience and patient survival after out-of-hospital tracheal intubation.
Methods: We analyzed probabilistically linked Pennsylvania statewide emergency medicine services, hospital discharge, and death data of patients receiving out-of-hospital tracheal intubation. We defined tracheal intubation experience as cumulative tracheal intubation during 2000 to 2005; low=1 to 10 tracheal intubations, medium=11 to 25 tracheal intubations, high=26 to 50 tracheal intubations, and very high=greater than 50 tracheal intubations. We identified survival on hospital discharge of patients intubated during 2003 to 2005. Using generalized estimating equations, we evaluated the association between patient survival and out-of-hospital rescuer cumulative tracheal intubation experience, adjusted for clinical covariates.
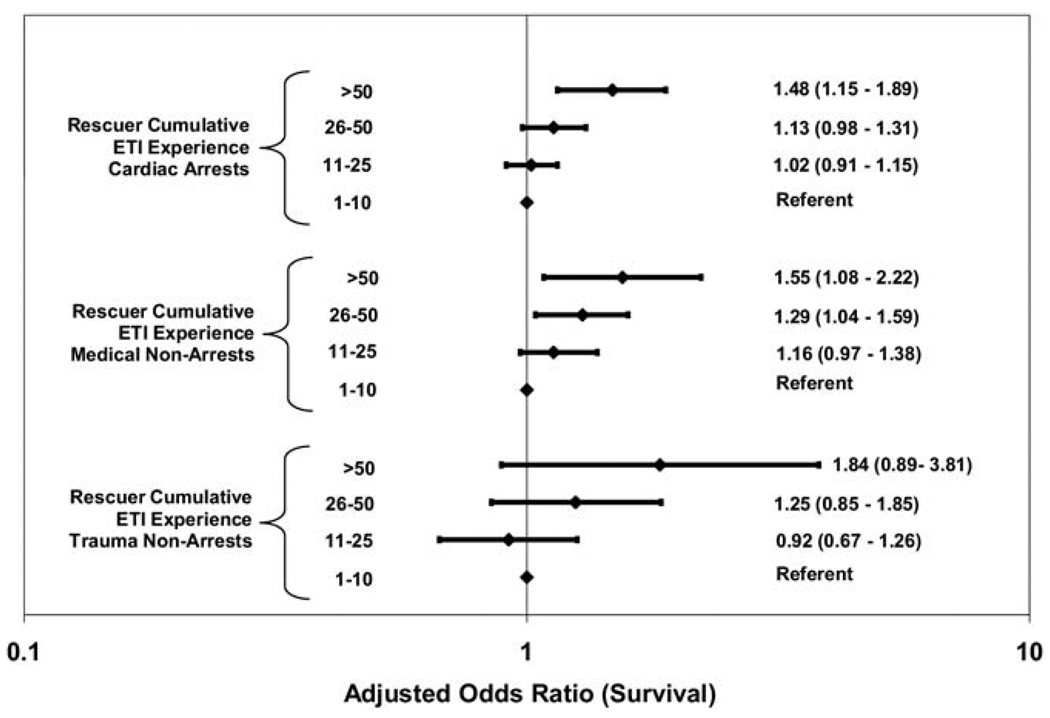
Results: During 2003 to 2005, 4,846 rescuers performed tracheal intubation. These individuals performed tracheal intubation on 33,117 patients during 2003 to 2005 and 62,586 patients during 2000 to 2005. Among 21,753 cardiac arrests, adjusted odds of survival was higher for patients intubated by rescuers with very high tracheal intubation experience; adjusted odds ratio (OR) versus low tracheal intubation experience: very high 1.48 (95% confidence interval [CI] 1.15 to 1.89), high 1.13 (95% CI 0.98 to 1.31), and medium 1.02 (95% CI 0.91 to 1.15). Among 8,162 medical nonarrests, adjusted odds of survival were higher for patients intubated by rescuers with high and very high tracheal intubation experience; adjusted OR versus low tracheal intubation experience: very high 1.55 (95% CI 1.08 to 2.22), high 1.29 (95% CI 1.04 to 1.59), and medium 1.16 (95% CI 0.97 to 1.38). Among 3,202 trauma nonarrests, survival was not associated with rescuer tracheal intubation experience; adjusted OR versus low tracheal intubation experience: very high 1.84 (95% CI 0.89 to 3.81), high 1.25 (95% CI 0.85 to 1.85), and medium 0.92 (95% CI 0.67 to 1.26).
Conclusion: Rescuer procedural experience is associated with improved patient survival after out-of-hospital tracheal intubation of cardiac arrest and medical nonarrest patients. Rescuer procedural experience is not associated with patient survival after out-of-hospital tracheal intubation of trauma nonarrest patients.
Copyright (c) 2009 American College of Emergency Physicians. Published by Mosby, Inc. All rights reserved.
Conflict of interest statement
By
Figures
Similar articles
-
How would minimum experience standards affect the distribution of out-of-hospital endotracheal intubations?Ann Emerg Med. 2007 Sep;50(3):246-52. doi: 10.1016/j.annemergmed.2007.04.023. Epub 2007 Jun 27. Ann Emerg Med. 2007. PMID: 17597255
-
Association Between Tracheal Intubation During Adult In-Hospital Cardiac Arrest and Survival.JAMA. 2017 Feb 7;317(5):494-506. doi: 10.1001/jama.2016.20165. JAMA. 2017. PMID: 28118660 Free PMC article.
-
Effect of emergency medical technician-placed Combitubes on outcomes after out-of-hospital cardiopulmonary arrest.Prehosp Emerg Care. 2009 Oct-Dec;13(4):495-9. doi: 10.1080/10903120903144874. Prehosp Emerg Care. 2009. PMID: 19731162
-
Cardiac Arrests Associated With Tracheal Intubations in PICUs: A Multicenter Cohort Study.Crit Care Med. 2016 Sep;44(9):1675-82. doi: 10.1097/CCM.0000000000001741. Crit Care Med. 2016. PMID: 27071070
-
What is the impact of physicians in prehospital treatment for patients in need of acute critical care? - An overview of reviews.Int J Technol Assess Health Care. 2019 Jan;35(1):27-35. doi: 10.1017/S0266462318003616. Epub 2019 Feb 6. Int J Technol Assess Health Care. 2019. PMID: 30722802 Review.
Cited by
-
Multiple failed intubation attempts are associated with decreased success rates on the first rescue intubation in the emergency department: a retrospective analysis of multicentre observational data.Scand J Trauma Resusc Emerg Med. 2015 Jan 16;23:5. doi: 10.1186/s13049-014-0085-8. Scand J Trauma Resusc Emerg Med. 2015. PMID: 25700237 Free PMC article.
-
Design and implementation of the Resuscitation Outcomes Consortium Pragmatic Airway Resuscitation Trial (PART).Resuscitation. 2016 Apr;101:57-64. doi: 10.1016/j.resuscitation.2016.01.012. Epub 2016 Feb 2. Resuscitation. 2016. PMID: 26851059 Free PMC article. Clinical Trial.
-
Out-of-hospital endotracheal intubation experience, confidence and confidence-associated factors among Northern Japanese emergency life-saving technicians: a population-based cross-sectional study.BMJ Open. 2018 Jul 13;8(7):e021858. doi: 10.1136/bmjopen-2018-021858. BMJ Open. 2018. PMID: 30007929 Free PMC article.
-
Feasibility of LMA Supreme for airway management in unconscious patients by ALS paramedics.Scand J Trauma Resusc Emerg Med. 2015 Feb 26;23:24. doi: 10.1186/s13049-015-0105-3. Scand J Trauma Resusc Emerg Med. 2015. PMID: 25888519 Free PMC article.
-
CPR Guidance by an Emergency Physician via Video Call: A Simulation Study.Emerg Med Int. 2018 Nov 29;2018:1480726. doi: 10.1155/2018/1480726. eCollection 2018. Emerg Med Int. 2018. PMID: 30627442 Free PMC article.
References
-
- Jacobs LM, Berrizbeitia LD, Bennett B, et al. Endotracheal intubation in the prehospital phase of emergency medical care. JAMA. 1983;250:2175–2177. - PubMed
-
- Stewart RD, Paris PM, Winter PM, et al. Field endotracheal intubation by paramedical personnel. Success rates and complications. Chest. 1984;85:341–345. - PubMed
-
- De Leo BC. Endotracheal intubation by rescue squad personnel. Heart Lung. 1977;6:851–854. - PubMed
-
- Guss DA, Posluszny M. Paramedic orotracheal intubation: a feasibility study. Am J Emerg Med. 1984;2:399–401. - PubMed
-
- Wang HE, Kupas DF, Greenwood MJ, et al. An algorithmic approach to prehospital airway management. Prehosp Emerg Care. 2005;9:145–155. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
