

Partners in crime: deregulation of AR activity and androgen synthesis in prostate cancer
- PMID: 20138542
- PMCID: PMC2862880
- DOI: 10.1016/j.tem.2010.01.002
Partners in crime: deregulation of AR activity and androgen synthesis in prostate cancer
Abstract
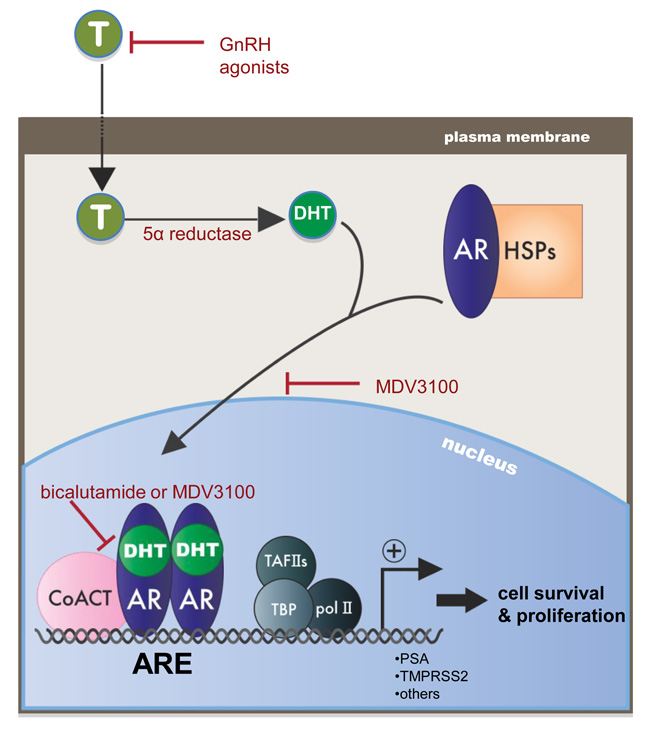
Prostate cancer remains a leading cause of cancer death, as there are no durable means to treat advanced disease. Treatment of non-organ-confined prostate cancer hinges on its androgen dependence. First-line therapeutic strategies suppress androgen receptor (AR) activity, via androgen ablation and direct AR antagonists, whereas initially effective, incurable, 'castration-resistant' tumors arise as a result of resurgent AR activity. Alterations of AR and/or associated regulatory networks are known to restore receptor activity and support resultant therapy-resistant tumor progression. However, recent evidence also reveals an unexpected contribution of the AR ligand, indicating that alterations in pathways controlling androgen synthesis support castration-resistant AR activity. In this report, the mechanisms underlying the lethal pairing of AR deregulation and aberrant androgen synthesis in prostate cancer progression will be discussed.
2010 Elsevier Ltd. All rights reserved.
Figures


References
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin. 2008;58:71–96. - PubMed
-
- Klein EA, Ciezki J, Kupelian PA, Mahadevan A. Outcomes for intermediate risk prostate cancer: Are there advantages for surgery, external radiation, or brachytherapy? Urol Oncol. 2009;27:67–71. - PubMed
-
- Klotz L. Combined androgen blockade: an update. Urol Clin North Am. 2006;33:161–166. v–vi. - PubMed
-
- Loblaw DA, Virgo KS, Nam R, et al. Initial hormonal management of androgen-sensitive metastatic, recurrent, or progressive prostate cancer: 2006 update of an American Society of Clinical Oncology practice guideline. J Clin Oncol. 2007;25:1596–1605. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
