

Cost effectiveness of management strategies for urinary tract infections: results from randomised controlled trial
- PMID: 20139218
- PMCID: PMC2817048
- DOI: 10.1136/bmj.c346
Cost effectiveness of management strategies for urinary tract infections: results from randomised controlled trial
Abstract
Objective: To assess the cost effectiveness of different management strategies for urinary tract infections.
Design: Cost effectiveness analysis alongside a randomised controlled trial with a one month follow-up.
Setting: Primary care.
Participants: 309 non-pregnant adult women aged 18-70 presenting with suspected urinary tract infection.
Interventions: Patients were randomised to five basic management approaches: empirical antibiotics, empirical delayed (by 48 hours) antibiotics, or targeted antibiotics based on either a high symptom score (two or more of urine cloudiness, smell, nocturia, dysuria), dipstick results (nitrite or leucocytes and blood), or receipt of a positive result on midstream urine analysis.
Main outcome measure: Duration of symptoms and cost of care.
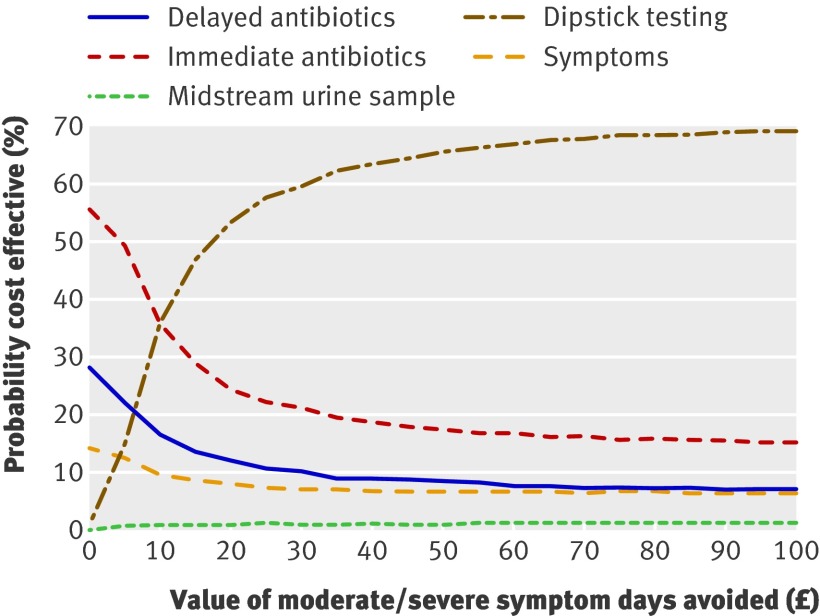
Results: Management with targeted antibiotics with midstream urine analysis was more costly over the period of one month. Costs for the midstream urine analysis and dipstick management groups were pound37 and pound35, respectively; these compared with pound31 for immediate antibiotics. Cost effectiveness acceptability curves suggested that if avoiding a day of moderately bad symptoms was valued at less than pound10, then immediate antibiotics is likely to be the most cost effective strategy. For values over pound10, targeted antibiotics with dipstick testing becomes the most cost effective strategy, though because of the uncertainty we can never be more than 70% certain that this strategy truly is the most cost effective.
Conclusion: Dipstick testing with targeted antibiotics is likely to be cost effective if the value of saving a day of moderately bad symptoms is pound10 or more, but caution is required given the considerable uncertainty surrounding the estimates.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
References
-
- HMSO, OPCS. Morbidity statistics from general practice: fourth national study 1991. HMSO, 1991.
-
- Foxman B. Epidemiology of urinary tract infections: incidence, morbidity, and economic costs. Dis Mon 2003;49:53-70. - PubMed
-
- Little P, Moore M, Turner S, Rumsby K, Warner G, Lowes A, et al. Effectiveness of five different approaches in the management of urinary tract infection: a randomised controlled trial. BMJ 2010. 10.1136/bmj.c199. - DOI - PMC - PubMed
-
- Curtis L, Netten A. Unit costs of health and social care. University of Kent, 2006. http://www.pssru.ac.uk/uc/uc2006contents.htm.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials