

Photorefractive keratectomy for the treatment of purely refractive accommodative esotropia: 6 years' experience
- PMID: 20139292
- PMCID: PMC2992963
- DOI: 10.1136/bjo.2009.160218
Photorefractive keratectomy for the treatment of purely refractive accommodative esotropia: 6 years' experience
Abstract
Aims: To report the long term outcomes of photorefractive keratectomy (PRK) for the treatment of hyperopia associated with purely refractive accommodative esotropia.
Methods: This study was a retrospective chart review of 40 patients aged 17-39 years who underwent PRK to eliminate their dependence on glasses. Pre- and postoperative best spectacle corrected visual acuity (BSCVA), uncorrected visual acuity (UCVA), refractive spherical equivalent (SEQ), ocular alignment and stereoacuity were reviewed.
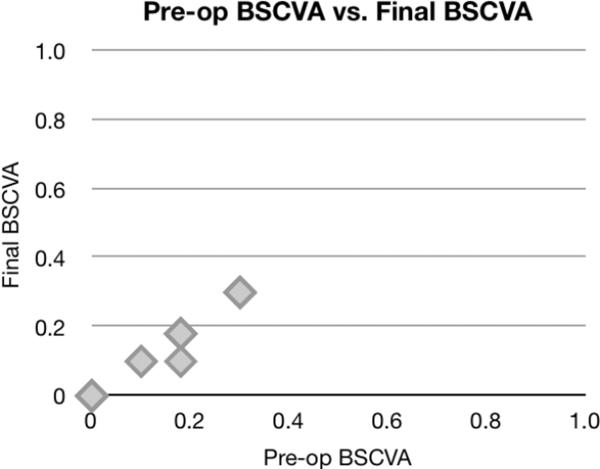
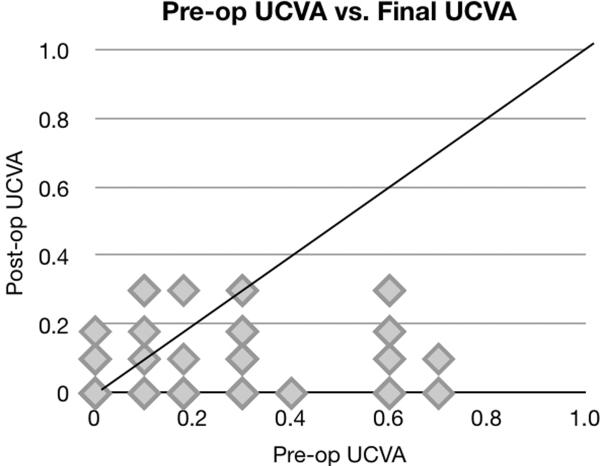
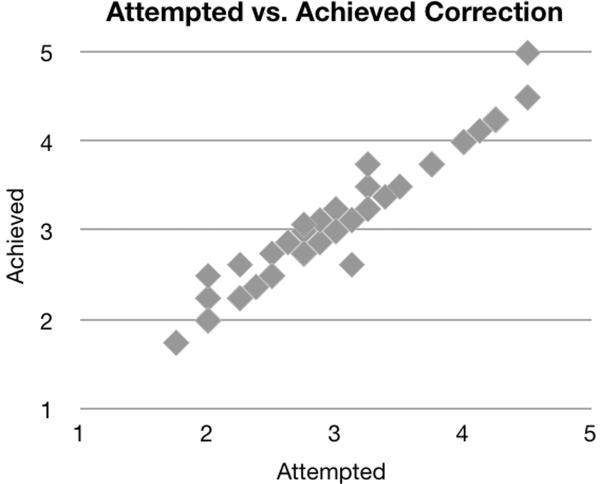
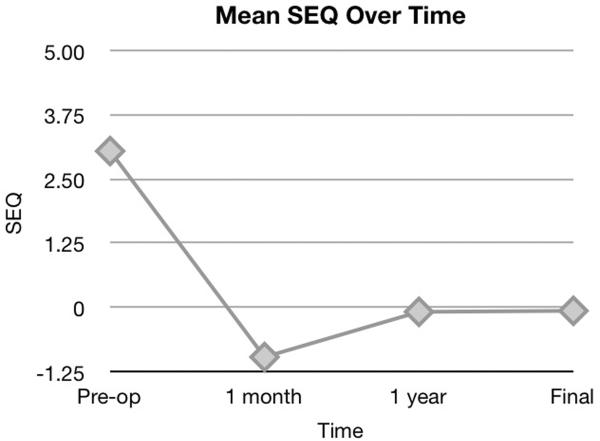
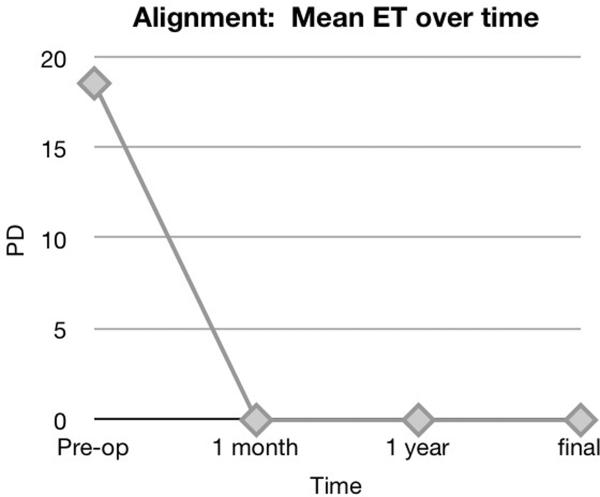
Results: Forty patients (80 eyes) with a mean age of 27.9 years were treated for a mean preoperative SEQ of +3.06 D hyperopia. The mean final postoperative SEQ was +0.06 D. Preoperative BSCVA was 0.04 logarithm of the minimum angle of resolution (logMAR), and did not change postoperatively. Mean UCVA significantly improved from 0.30 logMAR preoperatively to 0.08 logMAR post-operatively. Mean pre-operative esotropia at distance and near was 18.6 prism D. All patients were orthophoric without correction at the 1 month, 1 year and final postoperative evaluations. Visual acuity, refractive error and alignment remained stable after the 1 year postoperative examination. Stereoacuity was unchanged in 80% of patients postoperatively. There were no complications.
Conclusion: PRK can be used to treat low to moderate hyperopia associated with purely refractive accommodative esotropia in young adults.
Figures
Similar articles
-
Photorefractive keratectomy for the treatment of purely refractive accommodative esotropia.J Cataract Refract Surg. 2003 May;29(5):889-94. doi: 10.1016/s0886-3350(03)00011-7. J Cataract Refract Surg. 2003. PMID: 12781271
-
Photorefractive keratectomy on purely refractive accommodative esotropia.Semin Ophthalmol. 2015 Jan;30(1):25-8. doi: 10.3109/08820538.2013.810286. Epub 2013 Aug 16. Semin Ophthalmol. 2015. PMID: 23952080
-
Accommodative Esotropia Treatment Plan Utilizing Simultaneous Strabismus Surgery and Photorefractive Keratectomy.Am J Ophthalmol. 2018 Mar;187:125-129. doi: 10.1016/j.ajo.2018.01.005. Epub 2018 Jan 12. Am J Ophthalmol. 2018. PMID: 29339065
-
Wavefront excimer laser refractive surgery for adults with refractive errors.Cochrane Database Syst Rev. 2020 Dec 18;12(12):CD012687. doi: 10.1002/14651858.CD012687.pub2. Cochrane Database Syst Rev. 2020. PMID: 33336797 Free PMC article.
-
Refractive Surgery for Older Children and Adults with Accommodative Esotropia: A Systematic Review.Ophthalmic Res. 2022;65(4):361-376. doi: 10.1159/000523816. Epub 2022 Feb 28. Ophthalmic Res. 2022. PMID: 35226900
Cited by
-
LASIK as an alternative line to treat noncompliant esotropic children.Clin Ophthalmol. 2011;5:1795-801. doi: 10.2147/OPTH.S26827. Epub 2011 Dec 20. Clin Ophthalmol. 2011. PMID: 22267914 Free PMC article.
-
Photorefractive keratectomy influences the angle of ocular deviation in strabismus patients with hyperopia.Int Ophthalmol. 2019 Apr;39(4):737-744. doi: 10.1007/s10792-018-0867-5. Epub 2018 Mar 3. Int Ophthalmol. 2019. PMID: 29502213
-
Impact of laser refractive surgery on ocular alignment in myopic patients.Eye (Lond). 2014 Nov;28(11):1321-7. doi: 10.1038/eye.2014.209. Epub 2014 Sep 5. Eye (Lond). 2014. PMID: 25190533 Free PMC article.
-
Prognostic factors for stereopsis in refractive accommodative esotropia.Pak J Med Sci. 2015 Jul-Aug;31(4):807-11. doi: 10.12669/pjms.314.7465. Pak J Med Sci. 2015. PMID: 26430408 Free PMC article.
-
Accommodative esotropia: the state of the art.Int Ophthalmol. 2019 Feb;39(2):497-505. doi: 10.1007/s10792-018-0821-6. Epub 2018 Jan 13. Int Ophthalmol. 2019. PMID: 29332227 Review.
References
-
- Bilgihan K, Akata F, Or M, Hasanreisoglu B. Photorefractive keratectomy in refractive accommodative esotropia. Eye. 1997;11(Pt 3):409–10. - PubMed
-
- Farahi A, Hashemi H. The effect of hyperopic laser in situ keratomileusis on refractive accommodative esotropia. European Journal of Ophthalmology. 2005;15(6):688–94. - PubMed
-
- Hoyos JE, Cigales M, Hoyos-Chacon J, et al. Hyperopic laser in situ keratomileusis for refractive accommodative esotropia. Journal of Cataract & Refractive Surgery. 2002;28(9):1522–9. - PubMed
-
- Nucci P, Serafino M, Hutchinson AK. Photorefractive keratectomy for the treatment of purely refractive accommodative esotropia. Journal of Cataract & Refractive Surgery. 2003;29(5):889–94. - PubMed
-
- Nucci P, Serafino M, Hutchinson AK. Photorefractive keratectomy followed by strabismus surgery for the treatment of partly accommodative esotropia. Journal of Aapos: American Association for Pediatric Ophthalmology & Strabismus. 2004;8(6):555–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources