

Can Alzheimer disease be prevented by amyloid-beta immunotherapy?
- PMID: 20140000
- PMCID: PMC2864089
- DOI: 10.1038/nrneurol.2009.219
Can Alzheimer disease be prevented by amyloid-beta immunotherapy?
Erratum in
- Nat Rev Neurol. 2010 Apr;6(4):183
- Nat Rev Neurol. 2010 Jun;6(6):296
Abstract
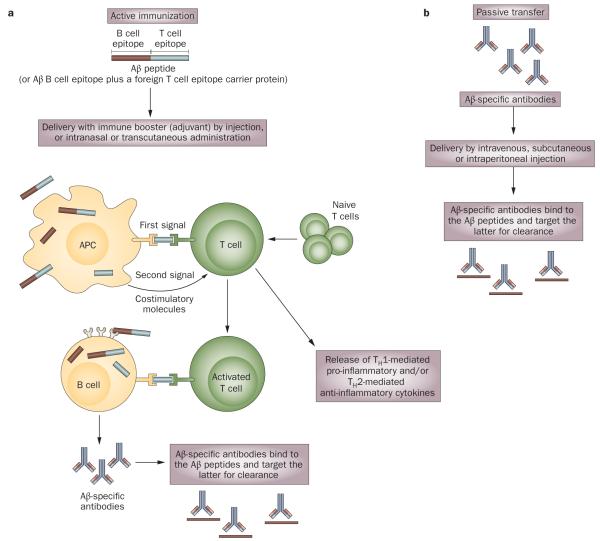
Alzheimer disease (AD) is the most common form of dementia. The amyloid-beta (Abeta) peptide has become a major therapeutic target in AD on the basis of pathological, biochemical and genetic evidence that supports a role for this molecule in the disease process. Active and passive Abeta immunotherapies have been shown to lower cerebral Abeta levels and improve cognition in animal models of AD. In humans, dosing in the phase II clinical trial of the AN1792 Abeta vaccine was stopped when approximately 6% of the immunized patients developed meningoencephalitis. However, some plaque clearance and modest clinical improvements were observed in patients following immunization. As a result of this study, at least seven passive Abeta immunotherapies are now in clinical trials in patients with mild to moderate AD. Several second-generation active Abeta vaccines are also in early clinical trials. On the basis of preclinical studies and the limited data from clinical trials, Abeta immunotherapy might be most effective in preventing or slowing the progression of AD when patients are immunized before or in the very earliest stages of disease onset. Biomarkers for AD and imaging technology have improved greatly over the past 10 years and, in the future, might be used to identify presymptomatic, at-risk individuals who might benefit from Abeta immunization.
Figures

References
-
- Brookmeyer R, Johnson E, Ziegler-Graham K, Arrighi H. Forecasting the global burden of Alzheimer’s disease. Alzheimers Dement. 2007;3:186–191. - PubMed
-
- Dickson DW. The pathogenesis of senile plaques. J. Neuropathol. Exp. Neurol. 1997;56:321–339. - PubMed
-
- Hardy J, Selkoe DJ. The amyloid hypothesis of Alzheimer’s disease: progress and problems on the road to therapeutics. Science. 2002;297:353–356. - PubMed
-
- Wolfe MS. Shutting down Alzheimer’s. Sci. Am. 2006;294:72–79. - PubMed
-
- Selkoe DJ. Alzheimer’s disease: genes, proteins, and therapy. Physiol. Rev. 2001;81:741–766. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
