

Warfarin pharmacogenomics
Abstract
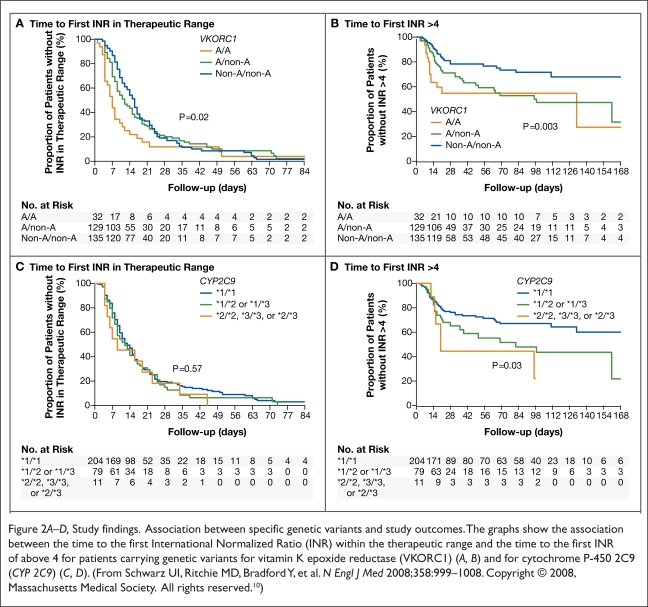
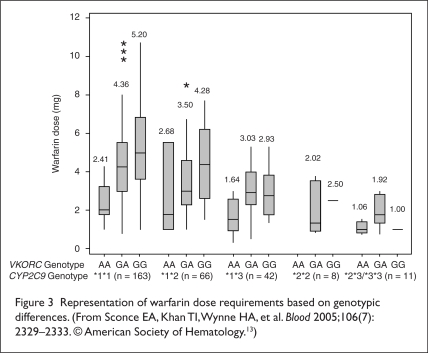
Warfarin, an anticoagulant, is used to prevent and treat thromboembolic disease. One of the drawbacks of this agent, also known as Coumadin (Bristol-Myers Squibb), is that it is difficult to administer at the correct dose as a result of its narrow therapeutic index, its tendency to cause bleeding, and the individual variability in patient response. Achieving safe and effective doses of warfarin therapy is both an urgent and important concern for many clinicians.Recent research has focused on single-nucleotide polymorphisms (SNPs) of genes that encode two proteins: the cytochrome P450 2C9 enzyme and VKORC1 (vitamin K epoxide reductase complex). Studies suggest that CYP 2C9 influences warfarin metabolism, whereas VKORC1 plays a role in the pharmacodynamic response in expression of the enzymatic target of warfarin. Patients who carry CYP 2C9*2 and CYP 2C9*3 alleles tend to require lower warfarin maintenance doses because of their slowed metabolism compared with patients who carry the "wild-type" allele. Patients who carry the VKORC1 A haplotype tend to require lower wafarin maintenance doses as a result of a decreased expression of messenger RNA (mRNA), which produces the proteins necessary for the formation of VKORC1.
Figures

References
-
- Shurin SB, Nabel EG. Pharmacogenomics: Ready for prime time? N Engl J Med. 2008;358(10):1061–1063. - PubMed
-
- Kamali F, King BP, Frearson R, et al. Contribution of age, body size, and CYP2C9 genotype to anticoagulant response to warfarin. Clin Pharmacol Ther. 2004;75:204–212. - PubMed
-
- Schwarz UI, Stein CM. Genetic determinants of dose and clinical outcomes in patients receiving oral anticoagulants. Clin Pharmacol Ther. 2006;80:7–12. - PubMed
-
- Zhu Y, Shennan M, Reynolds KK, et al. Estimation of warfarin maintenance dose based on VKORC1 (−1639 G>A) and CYP 2C9 genotypes. Clin Chem. 2007;53(7):1199–1205. - PubMed
-
- Rettie AE, Tai GY. The pharmacogenomics of warfarin: Closing in on personalized medicine. Mol Interv. 2006;6(4):223–226. - PubMed
LinkOut - more resources
Full Text Sources