

Differential patterns of infection and disease with P. falciparum and P. vivax in young Papua New Guinean children
- PMID: 20140220
- PMCID: PMC2816213
- DOI: 10.1371/journal.pone.0009047
Differential patterns of infection and disease with P. falciparum and P. vivax in young Papua New Guinean children
Abstract
Background: Where P. vivax and P. falciparum occur in the same population, the peak burden of P. vivax infection and illness is often concentrated in younger age groups. Experiences from malaria therapy patients indicate that immunity is acquired faster to P. vivax than to P. falciparum challenge. There is however little prospective data on the comparative risk of infection and disease from both species in young children living in co-endemic areas.
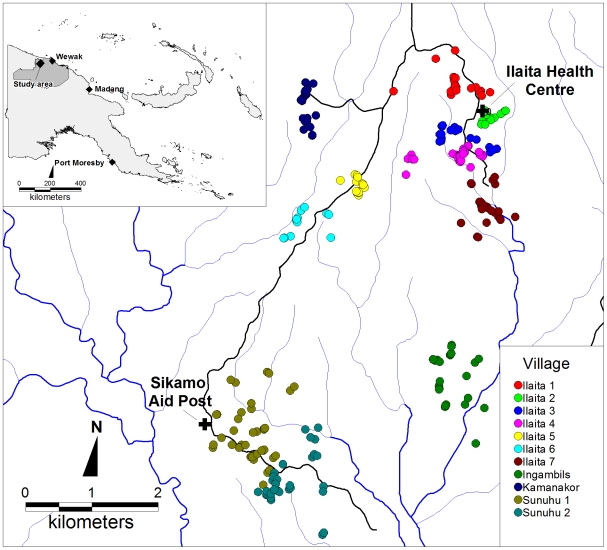
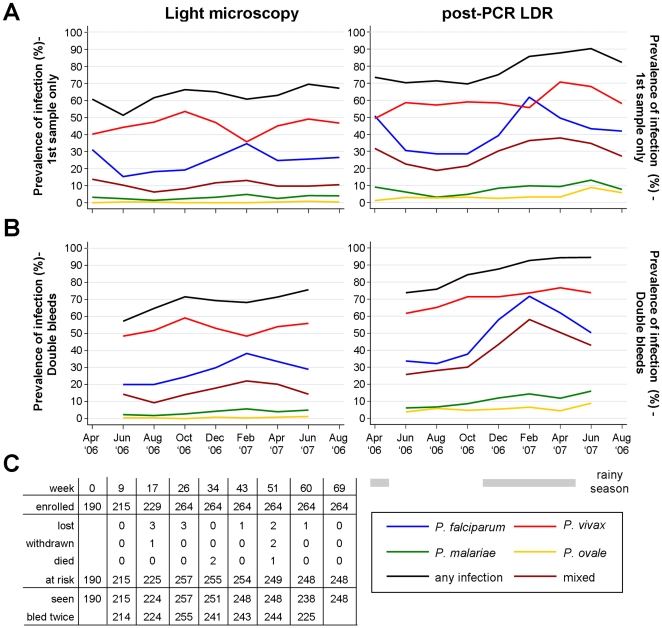
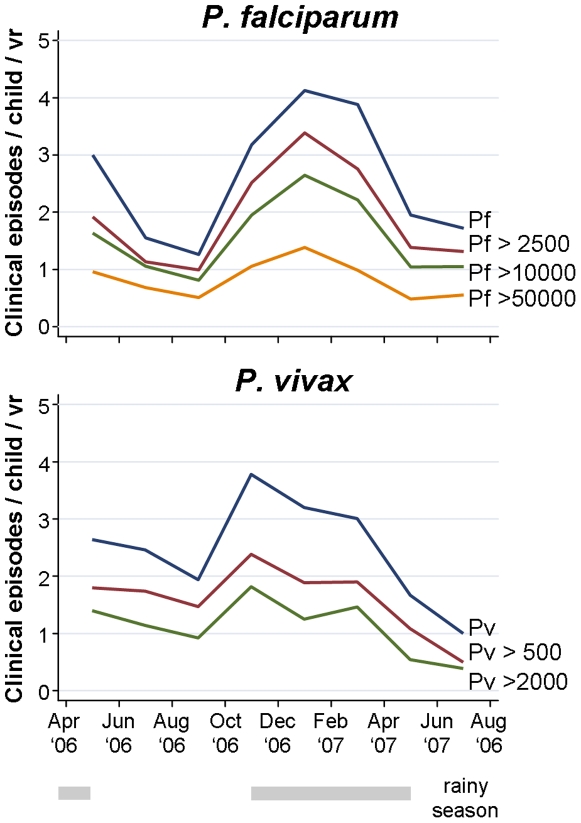
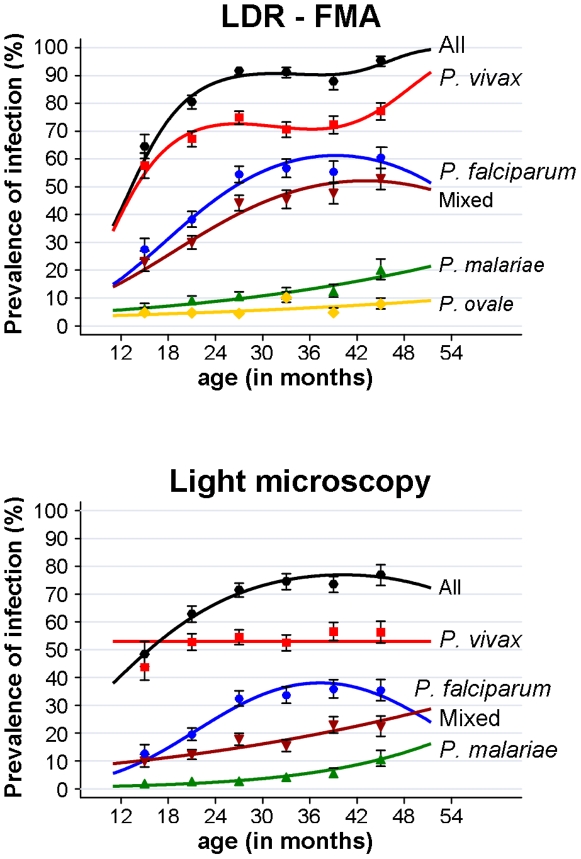
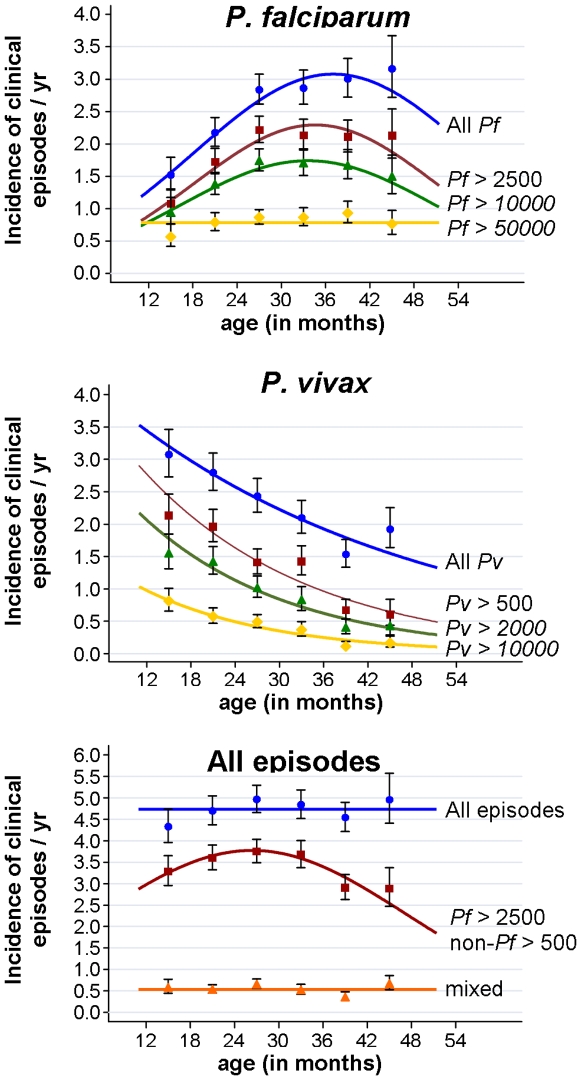
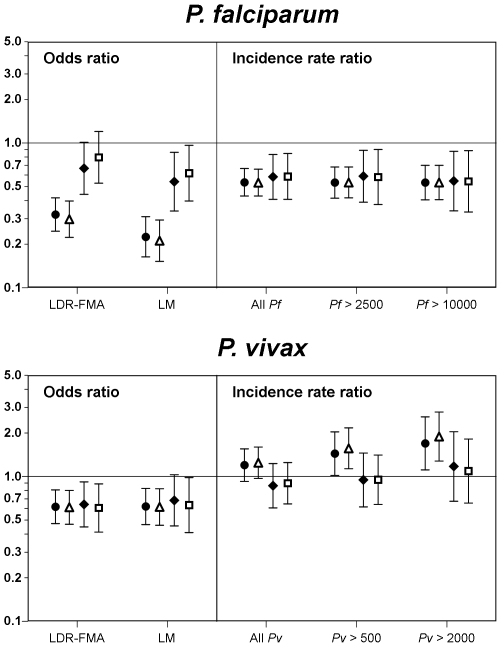
Methodology/principal findings: A cohort of 264 Papua New Guinean children aged 1-3 years (at enrolment) were actively followed-up for Plasmodium infection and febrile illness for 16 months. Infection status was determined by light microscopy and PCR every 8 weeks and at each febrile episode. A generalised estimating equation (GEE) approach was used to analyse both prevalence of infection and incidence of clinical episodes. A more pronounced rise in prevalence of P. falciparum compared to P. vivax infection was evident with increasing age. Although the overall incidence of clinical episodes was comparable (P. falciparum: 2.56, P. vivax 2.46 episodes / child / yr), P. falciparum and P. vivax infectious episodes showed strong but opposing age trends: P. falciparum incidence increased until the age of 30 months with little change thereafter, but incidence of P. vivax decreased significantly with age throughout the entire age range. For P. falciparum, both prevalence and incidence of P. falciparum showed marked seasonality, whereas only P. vivax incidence but not prevalence decreased in the dry season.
Conclusions/significance: Under high, perennial exposure, children in PNG begin acquiring significant clinical immunity, characterized by an increasing ability to control parasite densities below the pyrogenic threshold to P. vivax, but not to P. falciparum, in the 2(nd) and 3(rd) year of life. The ability to relapse from long-lasting liver-stages restricts the seasonal variation in prevalence of P. vivax infections.
Conflict of interest statement
Figures
Similar articles
-
The Incidence and Differential Seasonal Patterns of Plasmodium vivax Primary Infections and Relapses in a Cohort of Children in Papua New Guinea.PLoS Negl Trop Dis. 2016 May 4;10(5):e0004582. doi: 10.1371/journal.pntd.0004582. eCollection 2016 May. PLoS Negl Trop Dis. 2016. PMID: 27144482 Free PMC article.
-
Differential impact of malaria control interventions on P. falciparum and P. vivax infections in young Papua New Guinean children.BMC Med. 2019 Dec 9;17(1):220. doi: 10.1186/s12916-019-1456-9. BMC Med. 2019. PMID: 31813381 Free PMC article.
-
The risk of malarial infections and disease in Papua New Guinean children.Am J Trop Med Hyg. 2007 Jun;76(6):997-1008. Am J Trop Med Hyg. 2007. PMID: 17556601 Free PMC article.
-
Vaccines against malaria: perspectives from Papua New Guinea.Hum Vaccin. 2010 Jan;6(1):17-20. doi: 10.4161/hv.6.1.10332. Epub 2010 Jan 15. Hum Vaccin. 2010. PMID: 20173407 Review.
-
Malaria epidemiology and interventions in Ethiopia from 2001 to 2016.Infect Dis Poverty. 2018 Nov 5;7(1):103. doi: 10.1186/s40249-018-0487-3. Infect Dis Poverty. 2018. PMID: 30392470 Free PMC article. Review.
Cited by
-
Malaria and immunity during pregnancy and postpartum: a tale of two species.Parasitology. 2015 Jul;142(8):999-1015. doi: 10.1017/S0031182015000074. Epub 2015 Mar 3. Parasitology. 2015. PMID: 25731914 Free PMC article. Review.
-
Tolerability and safety of primaquine in Papua New Guinean children 1 to 10 years of age.Antimicrob Agents Chemother. 2012 Apr;56(4):2146-9. doi: 10.1128/AAC.05566-11. Epub 2012 Jan 17. Antimicrob Agents Chemother. 2012. PMID: 22252800 Free PMC article.
-
Plasmodium vivax Diversity and Population Structure across Four Continents.PLoS Negl Trop Dis. 2015 Jun 30;9(6):e0003872. doi: 10.1371/journal.pntd.0003872. eCollection 2015. PLoS Negl Trop Dis. 2015. PMID: 26125189 Free PMC article.
-
A comparative study of natural immune responses against Plasmodium vivax C-terminal merozoite surface protein-1 (PvMSP-1) and apical membrane antigen-1 (PvAMA-1) in two endemic settings.EXCLI J. 2015 Aug 6;14:926-34. doi: 10.17179/excli2015-388. eCollection 2015. EXCLI J. 2015. PMID: 26713085 Free PMC article.
-
Prevalence and proportion estimate of asymptomatic Plasmodium infection in Asia: a systematic review and meta-analysis.Sci Rep. 2023 Jun 27;13(1):10379. doi: 10.1038/s41598-023-37439-9. Sci Rep. 2023. PMID: 37369862 Free PMC article.
References
-
- Marsh K, Kinyanjui S. Immune effector mechanisms in malaria. Parasite Immunol. 2006;28:51–60. - PubMed
-
- Gupta S, Snow RW, Donnelly CA, Marsh K, Newbold C. Immunity to non-cerebral severe malaria is acquired after one or two infections. Nat Med. 1999;5:340–343. - PubMed
-
- Genton B, Al Yaman F, Beck HP, Hii J, Mellor S, et al. The epidemiology of malaria in the Wosera area, East Sepik Province, Papua New Guinea, in preparation for vaccine trials. I. Malariometric indices and immunity. Ann Trop Med Parasitol. 1995;89:359–376. - PubMed
-
- Genton B, Al Yaman F, Beck HP, Hii J, Mellor S, et al. The epidemiology of malaria in the Wosera area, East Sepik Province, Papua New Guinea, in preparation for vaccine trials. II. Mortality and morbidity. Ann Trop Med Parasitol. 1995;89:377–390. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
