

A comparison of echocardiography to invasive measurement in the evaluation of pulmonary arterial hypertension in a rat model
- PMID: 20140524
- PMCID: PMC2868165
- DOI: 10.1007/s10554-010-9596-1
A comparison of echocardiography to invasive measurement in the evaluation of pulmonary arterial hypertension in a rat model
Abstract
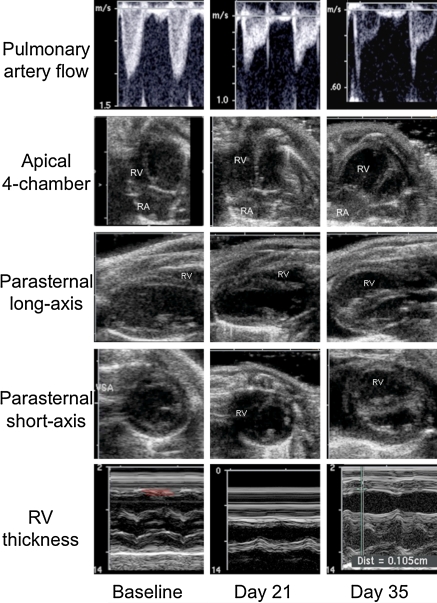
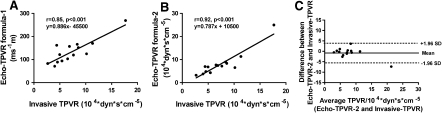
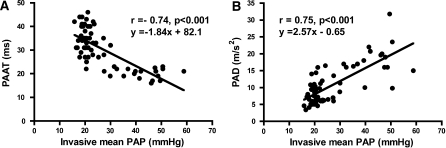
Pulmonary arterial hypertension (PAH) is a life-threatening condition characterized by progressive elevation in pulmonary artery pressure (PAP) and total pulmonary vascular resistance (TPVR). Recent advances in imaging techniques have allowed the development of new echocardiographic parameters to evaluate disease progression. However, there are no reports comparing the diagnostic performance of these non-invasive parameters to each other and to invasive measurements. Therefore, we investigated the diagnostic yield of echocardiographically derived TPVR and Doppler parameters of PAP in screening and measuring the severity of PAH in a rat model. Serial echocardiographic and invasive measurements were performed at baseline, 21 and 35 days after monocrotaline-induction of PAH. The most challenging echocardiographic derived TPVR measurement had good correlation with the invasive measurement (r = 0.92, P < 0.001) but also more simple and novel parameters of TPVR were found to be useful although the non-invasive TPVR measurement was feasible in only 29% of the studies due to lack of sufficient tricuspid valve regurgitation. However, echocardiographic measures of PAP, pulmonary artery flow acceleration time (PAAT) and deceleration (PAD), were measurable in all animals, and correlated with invasive PAP (r = -0.74 and r = 0.75, P < 0.001 for both). Right ventricular thickness and area correlated with invasive PAP (r = 0.59 and r = 0.64, P < 0.001 for both). Observer variability of the invasive and non-invasive parameters was low except in tissue-Doppler derived isovolumetric relaxation time. These non-invasive parameters may be used to replace invasive measurements in detecting successful disease induction and to complement invasive data in the evaluation of PAH severity in a rat model.
Figures
Comment in
-
Evaluation of pulmonary arterial hypertension: invasive or noninvasive?Int J Cardiovasc Imaging. 2011 Oct;27(7):943-5. doi: 10.1007/s10554-010-9642-z. Epub 2010 May 17. Int J Cardiovasc Imaging. 2011. PMID: 20473785 Free PMC article. No abstract available.
Similar articles
-
Two simple echo-Doppler measurements can accurately identify pulmonary hypertension in the large majority of patients with chronic heart failure.J Heart Lung Transplant. 2005 Jun;24(6):745-54. doi: 10.1016/j.healun.2004.03.026. J Heart Lung Transplant. 2005. PMID: 15949736
-
Noninvasive Echocardiographic Measures of Pulmonary Vascular Resistance in Children and Young Adults with Cardiomyopathy.J Am Soc Echocardiogr. 2018 Jul;31(7):807-815. doi: 10.1016/j.echo.2018.01.026. Epub 2018 Mar 27. J Am Soc Echocardiogr. 2018. PMID: 29602613
-
Validation of high-resolution echocardiography and magnetic resonance imaging vs. high-fidelity catheterization in experimental pulmonary hypertension.Am J Physiol Lung Cell Mol Physiol. 2010 Sep;299(3):L401-12. doi: 10.1152/ajplung.00114.2010. Epub 2010 Jun 25. Am J Physiol Lung Cell Mol Physiol. 2010. PMID: 20581101 Free PMC article.
-
Doppler flow patterns in the evaluation of pulmonary hypertension.Rom J Intern Med. 2009;47(2):109-21. Rom J Intern Med. 2009. PMID: 20067161 Review.
-
PATET ratio by Doppler echocardiography: noninvasive detection of pediatric pulmonary arterial hypertension.Pediatr Res. 2022 Sep;92(3):631-636. doi: 10.1038/s41390-021-01840-9. Epub 2021 Nov 18. Pediatr Res. 2022. PMID: 34795389 Free PMC article. Review.
Cited by
-
Activation of GPER ameliorates experimental pulmonary hypertension in male rats.Eur J Pharm Sci. 2017 Jan 15;97:208-217. doi: 10.1016/j.ejps.2016.11.009. Epub 2016 Nov 9. Eur J Pharm Sci. 2017. PMID: 27836751 Free PMC article.
-
DNA methyltransferase 3B deficiency unveils a new pathological mechanism of pulmonary hypertension.Sci Adv. 2020 Dec 9;6(50):eaba2470. doi: 10.1126/sciadv.aba2470. Print 2020 Dec. Sci Adv. 2020. PMID: 33298433 Free PMC article.
-
The Sugen 5416/hypoxia mouse model of pulmonary hypertension revisited: long-term follow-up.Pulm Circ. 2014 Dec;4(4):619-29. doi: 10.1086/678508. Pulm Circ. 2014. PMID: 25610598 Free PMC article.
-
Macitentan treatment retards the progression of established pulmonary arterial hypertension in an animal model.Int J Cardiol. 2014 Dec 15;177(2):423-8. doi: 10.1016/j.ijcard.2014.09.005. Epub 2014 Oct 11. Int J Cardiol. 2014. PMID: 25305681 Free PMC article.
-
Resveratrol Prevents Right Ventricle Remodeling and Dysfunction in Monocrotaline-Induced Pulmonary Arterial Hypertension with a Limited Improvement in the Lung Vasculature.Oxid Med Cell Longev. 2020 Feb 3;2020:1841527. doi: 10.1155/2020/1841527. eCollection 2020. Oxid Med Cell Longev. 2020. PMID: 32089765 Free PMC article.
References
-
- Simonneau G, Robbins IM, Beghetti M, Channick RN, Delcroix M, Denton CP, Elliott CG, Gaine SP, Gladwin MT, Jing ZC, Krowka MJ, Langleben D, Nakanishi N, Souza R. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2009;54:S43–S54. doi: 10.1016/j.jacc.2009.04.012. - DOI - PubMed
-
- D’Alonzo GE, Barst RJ, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, Fishman AP, Goldring RM, Groves BM, Kernis JT. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med. 1991;115:343–349. - PubMed
-
- Galie N, Hoeper MM, Humbert M, Torbicki A, Vachiery JL, Barbera JA, et al. Guidelines for the diagnosis and treatment of pulmonary hypertension: the task force for the diagnosis and treatment of pulmonary hypertension of the European society of cardiology (ESC) and the European respiratory society (ERS), endorsed by the International society of heart and lung transplantation (ISHLT) Eur Heart J. 2009;30:2493–2537. doi: 10.1093/eurheartj/ehp297. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
