

Uveitis in DiGeorge syndrome: a case of autoimmune ocular inflammation in a patient with deletion 22q11.2
- PMID: 20141355
- PMCID: PMC3009586
- DOI: 10.3109/13816810903426249
Uveitis in DiGeorge syndrome: a case of autoimmune ocular inflammation in a patient with deletion 22q11.2
Abstract
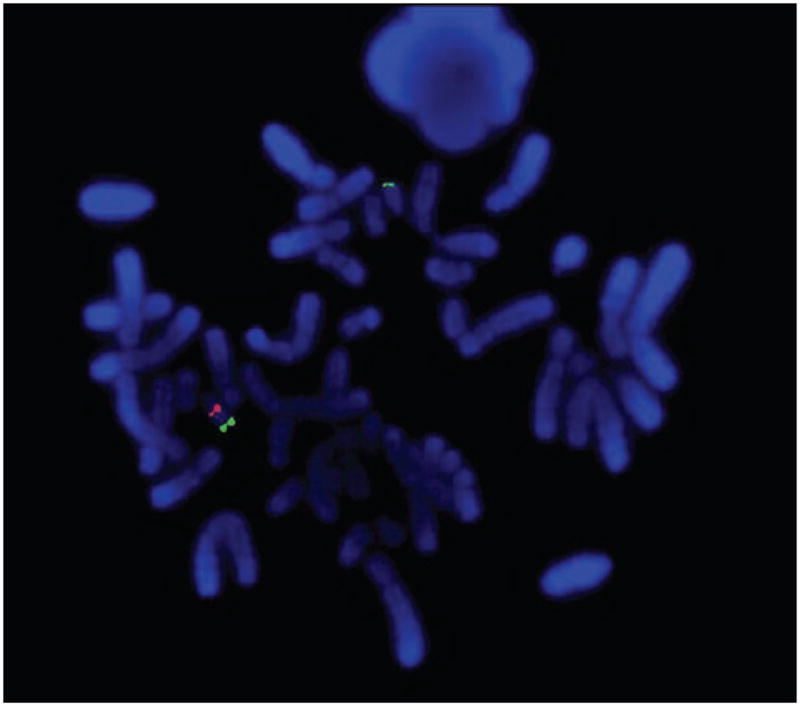
Purpose: Del22q11.2, also known as DiGeorge syndrome, has a spectrum of ocular, facial and systemic features. Despite features of T cell dysfunction, infection and autoimmunity (including juvenile idiopathic arthritis), uveitis has not been described in patients with DiGeorge syndrome.
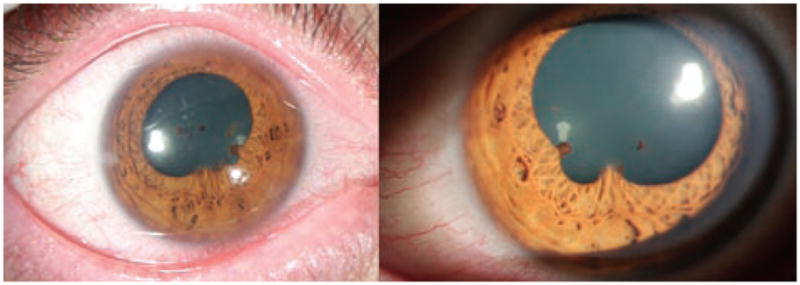
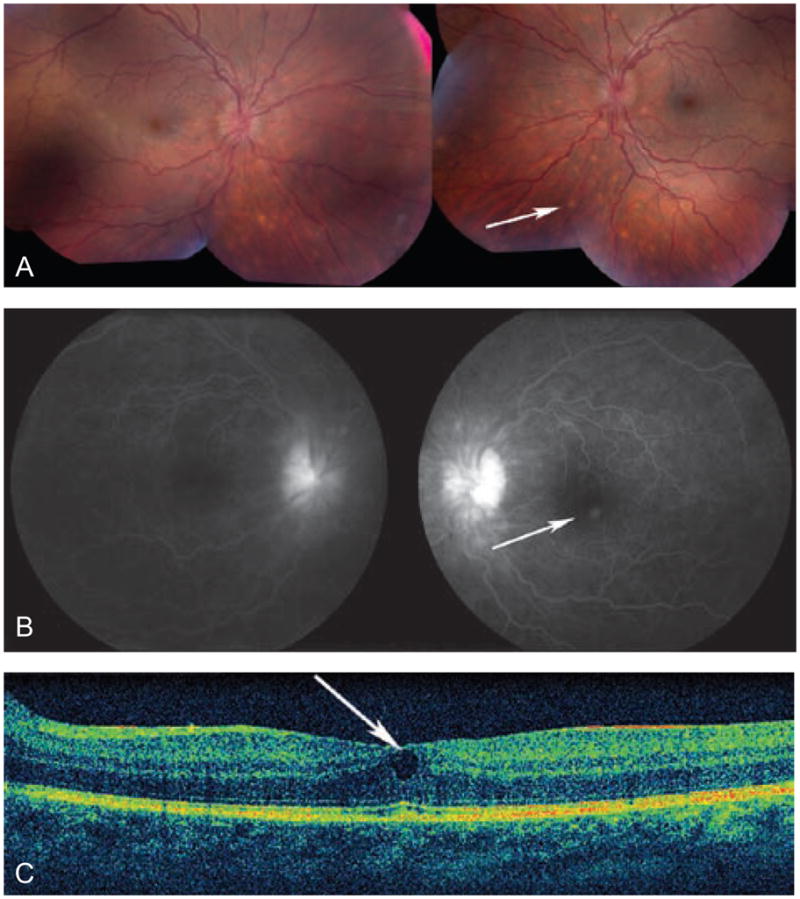
Methods: We describe a case of a 25-year-old male with bilateral granulomatous panuveitis who after initial investigation and treatment for an infectious cause was determined to have autoimmune-related uveitis with evidence on clinical, laboratory and imaging assessments suggestive of ocular sarcoidosis.
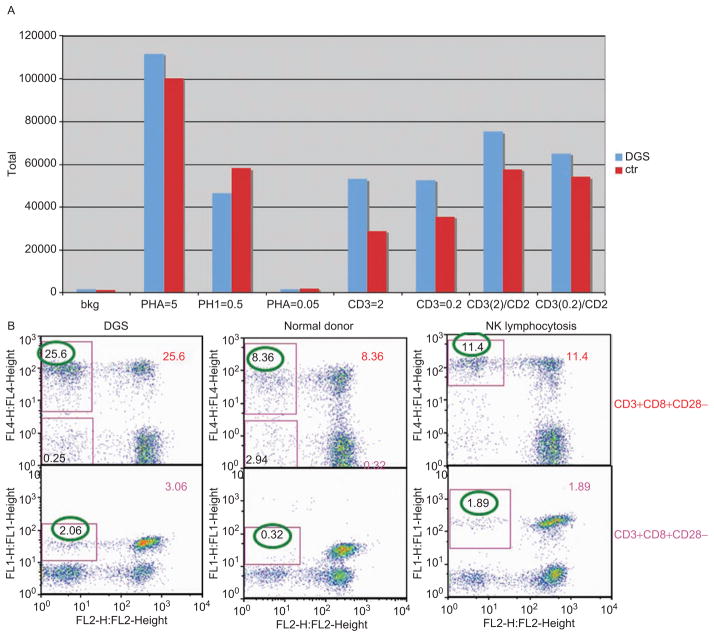
Results: The patient was found to have a normal T cell count and T cell proliferative response that was compared to a control patient, and phenotypes determined by flow cytometry were normal. However, the CD4/CD8 ratio in this patient was slightly lower than normal and the number of CD28 negative T cells, in both CD4 and CD8 populations, were significantly higher than a control.
Conclusions: The significance of these T cell abnormalities is unknown in the context of this patient's uveitis but is suggestive of a role in autoimmunity, which is a known phenomenon in del22q11.2 syndrome, although autoimmune-related uveitis is not a previously described feature.
Conflict of interest statement
Figures
Similar articles
-
Antibody deficiency and autoimmunity in 22q11.2 deletion syndrome.Arch Dis Child. 2002 Jun;86(6):422-5. doi: 10.1136/adc.86.6.422. Arch Dis Child. 2002. PMID: 12023174 Free PMC article.
-
[Clinical features and molecular diagnosis of three patients with DiGeorge anomaly].Zhonghua Er Ke Za Zhi. 2012 Dec;50(12):944-7. Zhonghua Er Ke Za Zhi. 2012. PMID: 23324155 Chinese.
-
Immunological aspects of 22q11.2 deletion syndrome.Cell Mol Life Sci. 2012 Jan;69(1):17-27. doi: 10.1007/s00018-011-0842-z. Epub 2011 Oct 9. Cell Mol Life Sci. 2012. PMID: 21984609 Free PMC article. Review.
-
Graves' disease in DiGeorge syndrome: patient report with a review of endocrine autoimmunity associated with 22q11.2 deletion.J Pediatr Endocrinol Metab. 2004 Nov;17(11):1575-9. doi: 10.1515/jpem.2004.17.11.1575. J Pediatr Endocrinol Metab. 2004. PMID: 15570997
-
Chromosome 22q11.2 deletion syndrome (DiGeorge and velocardiofacial syndromes).Curr Opin Pediatr. 2002 Dec;14(6):678-83. doi: 10.1097/00008480-200212000-00005. Curr Opin Pediatr. 2002. PMID: 12436034 Review.
Cited by
-
Ocular involvement in primary immunodeficiency diseases.J Clin Immunol. 2014 Jan;34(1):23-38. doi: 10.1007/s10875-013-9974-2. Epub 2013 Nov 30. J Clin Immunol. 2014. PMID: 24292697 Review.
-
Microphthalmia and orbital cysts in DiGeorge syndrome.J AAPOS. 2021 Dec;25(6):358-360. doi: 10.1016/j.jaapos.2021.06.001. Epub 2021 Sep 29. J AAPOS. 2021. PMID: 34597781 Free PMC article.
-
Pulmonary extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue associated with granulomatous inflammation in a child with chromosome 22q11.2 deletion syndrome (DiGeorge syndrome).J Pediatr. 2012 Nov;161(5):954-8. doi: 10.1016/j.jpeds.2012.07.003. Epub 2012 Aug 21. J Pediatr. 2012. PMID: 22920507 Free PMC article.
References
-
- Sullivan KE. Chromosome 22q11.2 deletion syndrome: DiGeorge syndrome/velocardiofacial Syndrome. Immunol Allergy Clin North Am. 2008;28(2):353–366. - PubMed
-
- Martin Mateos MA, Perez Duenas BP, Iriondo M, et al. Clinical and immunological spectrum of partial DiGeorge syndrome. J Investig Allergol Clin Immunol. 2000;10(6):352–360. - PubMed
-
- Greenberg F, Courtney KB, Wessels RA, et al. Prenatal diagnosis of deletion 17p13 associated with DiGeorge anomaly. Am J Med Genet. 1988;31(1):1–4. - PubMed
-
- DeBerardinis RJ, Medne L, Spinner NB, et al. DiGeorge anomaly in a patient with isochromosome 18p born to a diabetic mother. Am J Med Genet A. 2005;138A(2):155–159. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials