

Brain metabolism is significantly impaired at blood glucose below 6 mM and brain glucose below 1 mM in patients with severe traumatic brain injury
- PMID: 20141631
- PMCID: PMC2875528
- DOI: 10.1186/cc8869
Brain metabolism is significantly impaired at blood glucose below 6 mM and brain glucose below 1 mM in patients with severe traumatic brain injury
Abstract
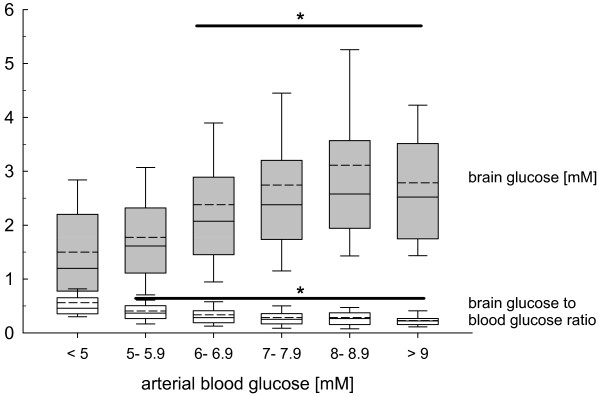
Introduction: The optimal blood glucose target following severe traumatic brain injury (TBI) must be defined. Cerebral microdialysis was used to investigate the influence of arterial blood and brain glucose on cerebral glucose, lactate, pyruvate, glutamate, and calculated indices of downstream metabolism.
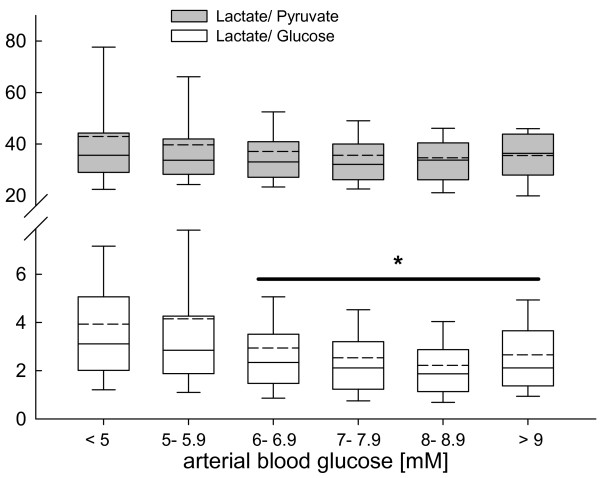
Methods: In twenty TBI patients, microdialysis catheters inserted in the edematous frontal lobe were dialyzed at 1 microl/min, collecting samples at 60 minute intervals. Occult metabolic alterations were determined by calculating the lactate- pyruvate (L/P), lactate- glucose (L/Glc), and lactate- glutamate (L/Glu) ratios.
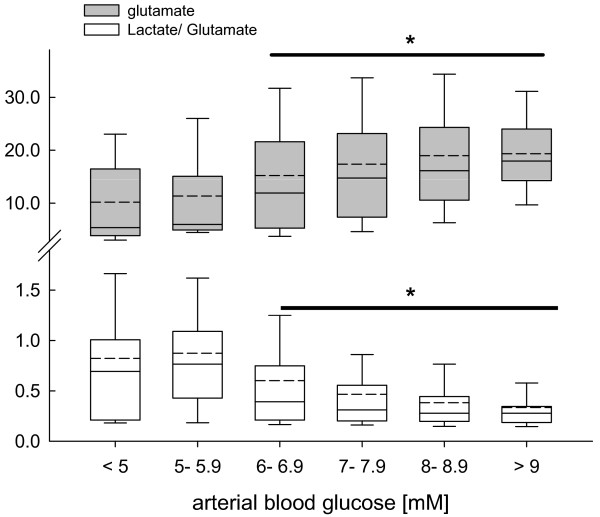
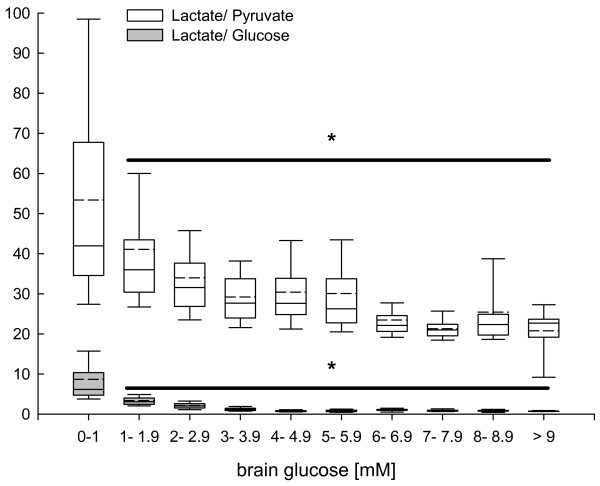
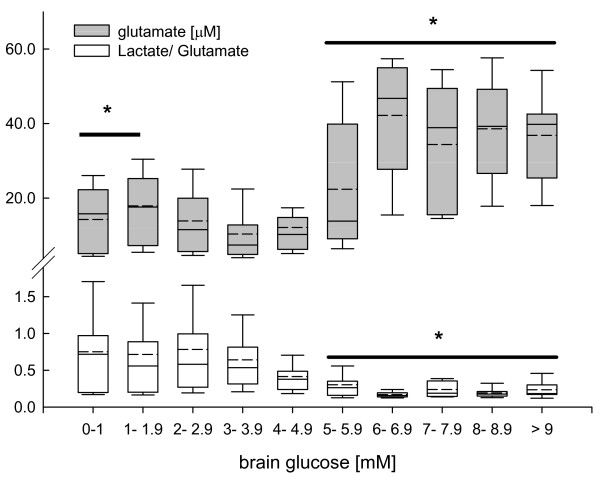
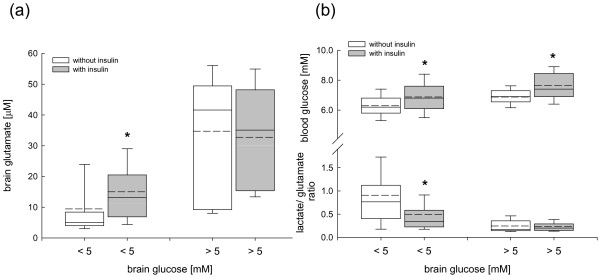
Results: Brain glucose was influenced by arterial blood glucose. Elevated L/P and L/Glc were significantly reduced at brain glucose above 1 mM, reaching lowest values at blood and brain glucose levels between 6-9 mM (P < 0.001). Lowest cerebral glutamate was measured at brain glucose 3-5 mM with a significant increase at brain glucose below 3 mM and above 6 mM. While L/Glu was significantly increased at low brain glucose levels, it was significantly decreased at brain glucose above 5 mM (P < 0.001). Insulin administration increased brain glutamate at low brain glucose, but prevented increase in L/Glu.
Conclusions: Arterial blood glucose levels appear to be optimal at 6-9 mM. While low brain glucose levels below 1 mM are detrimental, elevated brain glucose are to be targeted despite increased brain glutamate at brain glucose >5 mM. Pathogenity of elevated glutamate appears to be relativized by L/Glu and suggests to exclude insulin- induced brain injury.
Figures
Similar articles
-
Lactate shuttling and lactate use as fuel after traumatic brain injury: metabolic considerations.J Cereb Blood Flow Metab. 2014 Nov;34(11):1736-48. doi: 10.1038/jcbfm.2014.153. Epub 2014 Sep 10. J Cereb Blood Flow Metab. 2014. PMID: 25204393 Free PMC article. Review.
-
The frontal lobe and thalamus have different sensitivities to hypoxia-hypotension after traumatic brain injury: a microdialysis study in rats.J Neurotrauma. 2012 Dec 10;29(18):2782-90. doi: 10.1089/neu.2012.2381. Epub 2012 Sep 25. J Neurotrauma. 2012. PMID: 22860603
-
Impact of tight glycemic control on cerebral glucose metabolism after severe brain injury: a microdialysis study.Crit Care Med. 2008 Dec;36(12):3233-8. doi: 10.1097/CCM.0b013e31818f4026. Crit Care Med. 2008. PMID: 18936695
-
Cerebral extracellular chemistry and outcome following traumatic brain injury: a microdialysis study of 223 patients.Brain. 2011 Feb;134(Pt 2):484-94. doi: 10.1093/brain/awq353. Epub 2011 Jan 18. Brain. 2011. PMID: 21247930
-
[Use of intracerebral microdialysis in severe traumatic brain injury].No Shinkei Geka. 2010 Sep;38(9):795-809. No Shinkei Geka. 2010. PMID: 20864768 Review. Japanese.
Cited by
-
A meta-analysis of the effect of different neuroprotective drugs in management of patients with traumatic brain injury.Neurosurg Rev. 2018 Apr;41(2):427-438. doi: 10.1007/s10143-016-0775-y. Epub 2016 Aug 18. Neurosurg Rev. 2018. PMID: 27539610 Review.
-
Risk factors for hypoglycaemia in neurocritical care patients.Intensive Care Med. 2012 Dec;38(12):1999-2006. doi: 10.1007/s00134-012-2681-2. Epub 2012 Aug 21. Intensive Care Med. 2012. PMID: 22907674
-
Exogenous Ketones and Lactate as a Potential Therapeutic Intervention for Brain Injury and Neurodegenerative Conditions.Front Hum Neurosci. 2022 Apr 28;16:846183. doi: 10.3389/fnhum.2022.846183. eCollection 2022. Front Hum Neurosci. 2022. PMID: 36267349 Free PMC article. Review.
-
Rethinking the necessity of low glucose intervention for cerebral ischemia/reperfusion injury.Neural Regen Res. 2022 Jul;17(7):1397-1403. doi: 10.4103/1673-5374.330592. Neural Regen Res. 2022. PMID: 34916409 Free PMC article. Review.
-
Lactate shuttling and lactate use as fuel after traumatic brain injury: metabolic considerations.J Cereb Blood Flow Metab. 2014 Nov;34(11):1736-48. doi: 10.1038/jcbfm.2014.153. Epub 2014 Sep 10. J Cereb Blood Flow Metab. 2014. PMID: 25204393 Free PMC article. Review.
References
-
- Zygun DA, Steiner LA, Johnston AJ, Hutchinson PJ, Al-Rawi PG, Chatfield D, Kirkpatrick PJ, Menon DK, Gupta AK. Hyperglycemia and brain tissue pH after traumatic brain injury. Neurosurgery. 2004;55:877–881. - PubMed
-
- Diaz-Parejo P, Ståhl N, Xu W, Reinstrup P, Ungerstedt U, Nordström CH. Cerebral energy metabolism during transient hyperglycemia in patients with severe brain trauma. Intensive Care Med. 2003;29:544–550. - PubMed
-
- Jeremitsky E, Omert LA, Dunham CM, Wilberger J, Rodriguez A. The impact of hyperglycemia on patients with severe brain injury. J Trauma. 2005;58:47–50. - PubMed
-
- Aronson D. Hyperglycemia and the pathobiology of diabetic complications. Adv Cardiol. 2008;45:1–16. - PubMed
-
- Sperry JL, Frankel HL, Vanek SL, Nathens AB, Moore EE, Maier RV, Minei JP. Early hyperglycemia predicts multiple organ failure and mortality but not infection. J Trauma. 2007;63:487–493. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
