

Patient expectations from implantable defibrillators to prevent death in heart failure
- PMID: 20142021
- PMCID: PMC4497779
- DOI: 10.1016/j.cardfail.2009.09.003
Patient expectations from implantable defibrillators to prevent death in heart failure
Abstract
Background: Indications for implantable cardioverter-defibrillators (ICDs) in heart failure (HF) are expanding and may include more than 1 million patients. This study examined patient expectations from ICDs for primary prevention of sudden death in HF.
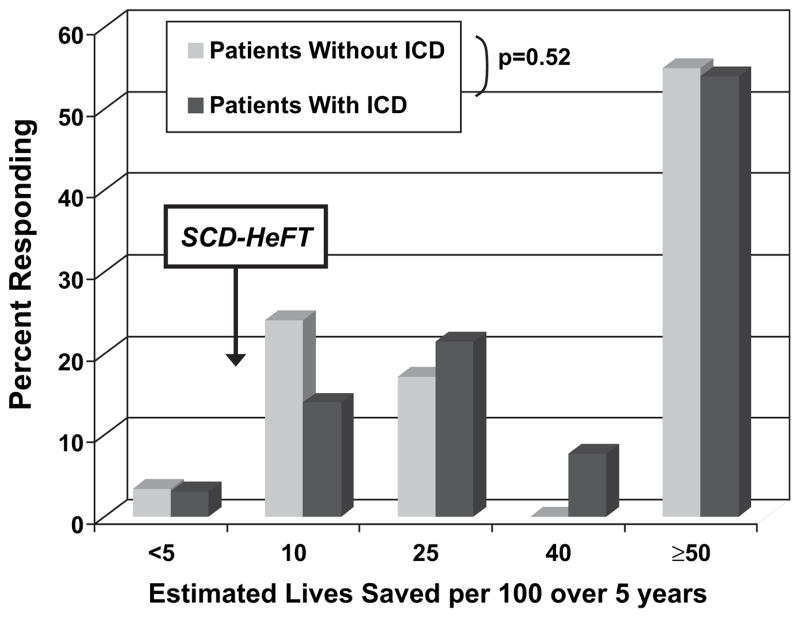
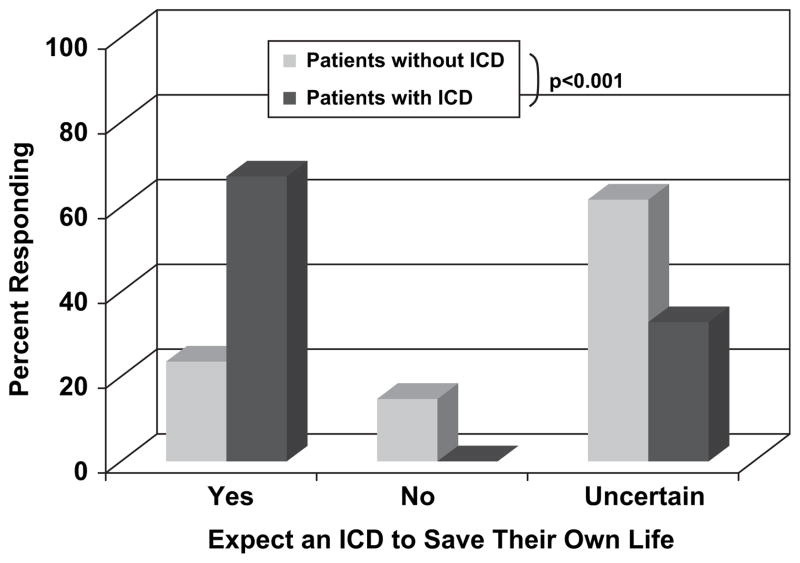
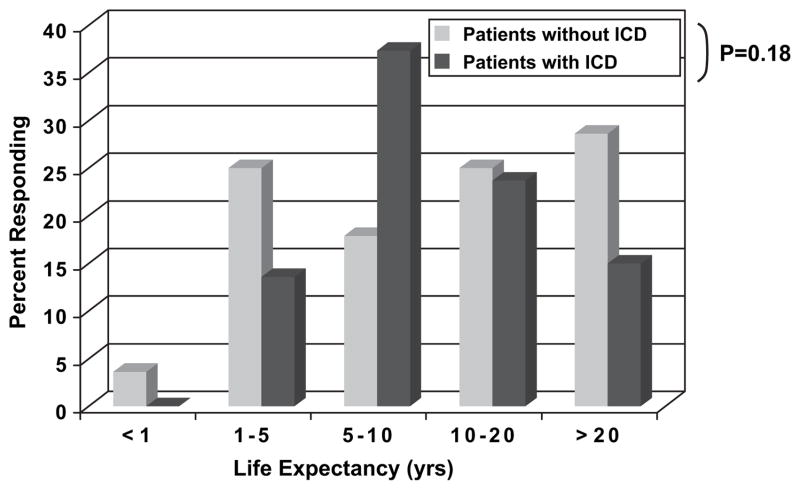
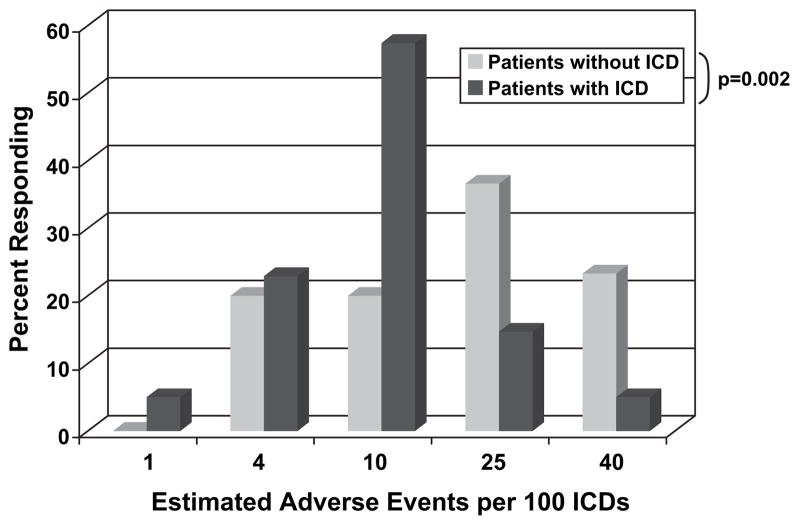
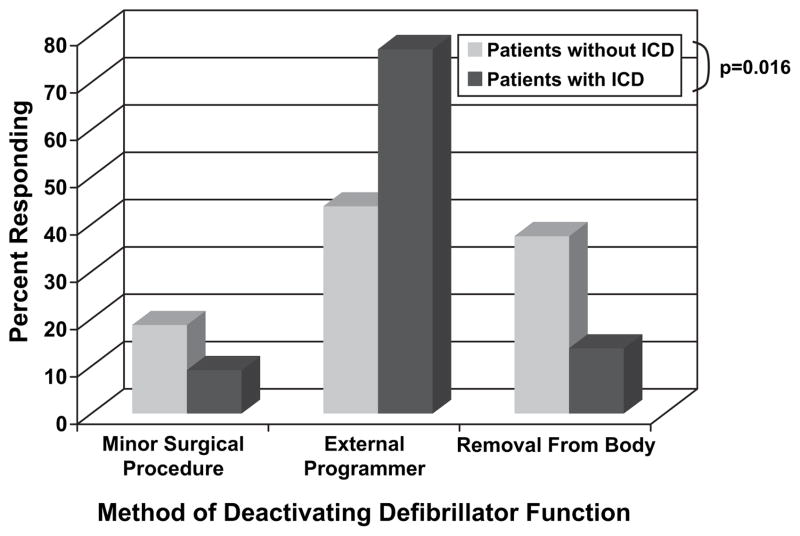
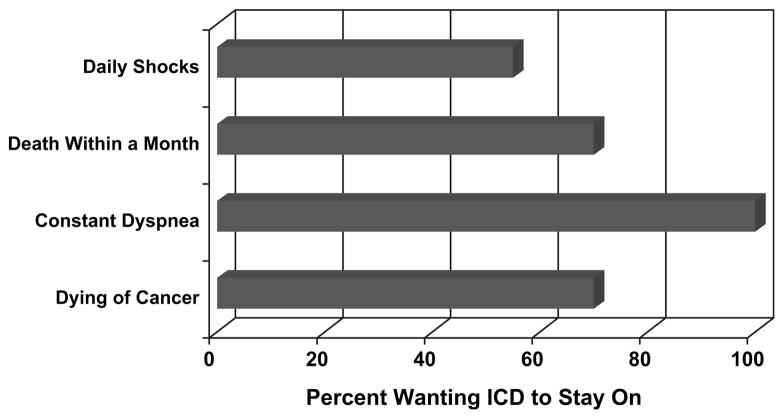
Methods and results: Study participants (n = 105) had an EF <35% and symptomatic HF, without history of ventricular tachycardia/fibrillation or syncope. Subjects completed a written survey about perceived ICD benefits, survival expectations, and circumstances under which they might deactivate defibrillation. Mean age was 58, LVEF 21%, 40% were New York Heart Association Class III-IV, and 65% already had a primary prevention ICD. Most patients anticipated more than10 years survival despite symptomatic HF. Nearly 54% expected an ICD to save >or=50 lives per 100 during 5 years. ICD recipients expressed more confidence that the device would save their own lives compared with those without an ICD (P < .001). Despite understanding the ease of deactivation, 70% of ICD recipients indicated they would keep the ICD on even if dying of cancer, 55% even if having daily shocks, and none would inactivate defibrillation even if suffering constant dyspnea at rest.
Conclusions: HF patients anticipate long survival, overestimate survival benefits conferred by ICDs, and express reluctance to deactivate their devices even for end-stage disease.
Copyright 2010 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interests: None.
Figures
References
-
- Hunt SA, Abraham WT, Chin MH, Feldman AM, Francis GS, Ganiats TG, et al. ACC/AHA 2005 Guideline Update for the Diagnosis and Management of Chronic Heart Failure in the Adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure): developed in collaboration with the American College of Chest Physicians and the International Society for Heart and Lung Transplantation: endorsed by the Heart Rhythm Society. Circulation. 2005;112:e154–235. - PubMed
-
- HFSA. 2006 Comprehensive Heart Failure Practice Guideline. J Cardiac Failure. 2006;12:e1–2. - PubMed
-
- Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R, et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005;352:225–37. - PubMed
-
- Hohnloser SH, Kuck KH, Dorian P, Roberts RS, Hampton JR, Hatala R, et al. Prophylactic use of an implantable cardioverter-defibrillator after acute myocardial infarction. N Engl J Med. 2004;351:2481–8. - PubMed
-
- Moss AJ, Zareba W, Hall WJ, Klein H, Wilber DJ, Cannom DS, et al. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. 2002;346:877–83. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
