

MRI of the corpus callosum in multiple sclerosis: association with disability
- PMID: 20142309
- PMCID: PMC2820126
- DOI: 10.1177/1352458509353649
MRI of the corpus callosum in multiple sclerosis: association with disability
Abstract
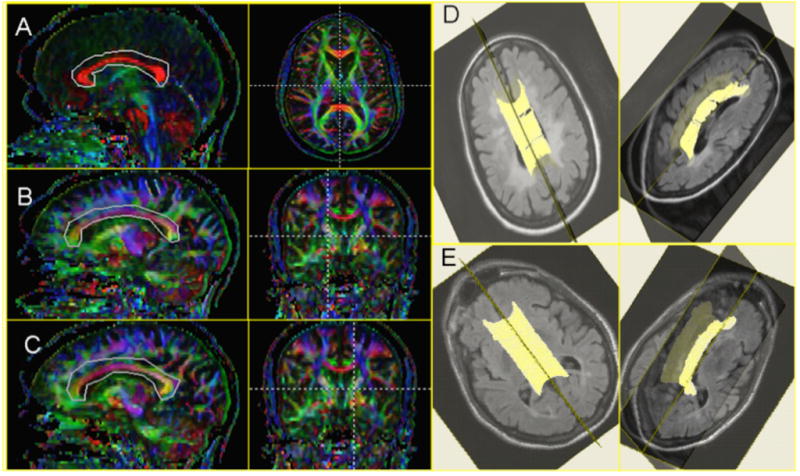
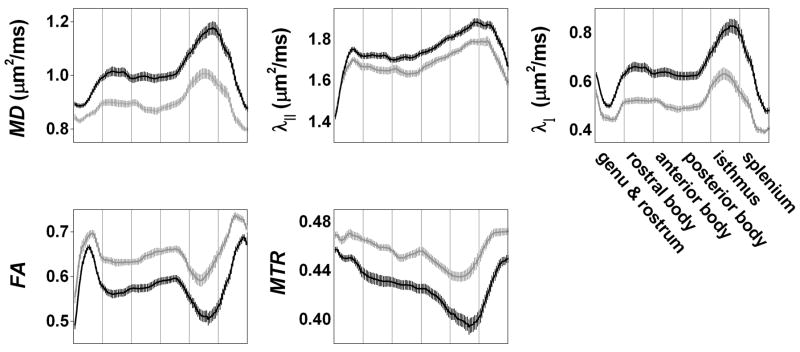
Inflammatory demyelination and axon damage in the corpus callosum are prominent features of multiple sclerosis (MS) and may partially account for impaired performance on complex tasks. The objective of this article was to characterize quantitative callosal MRI abnormalities and their association with disability. In 69 participants with MS and 29 healthy volunteers, lesional and extralesional callosal MRI indices were estimated via diffusion tensor tractography. expanded disability status scale (EDSS) and MS functional composite (MSFC) scores were recorded in 53 of the participants with MS. All tested callosal MRI indices were diffusely abnormal in MS. EDSS score was correlated only with age (r = 0.51). Scores on the overall MSFC and its paced serial auditory addition test (PASAT) and 9-hole peg test components were correlated with callosal fractional anisotropy (r = 0.27, 0.35, and 0.31, respectively) and perpendicular diffusivity (r = -0.29, -0.30, and -0.31) but not with overall callosal volume or callosal lesion volume; the PASAT score was more weakly correlated with callosal magnetization-transfer ratio (r = 0.21). Anterior callosal abnormalities were associated with impaired PASAT performance and posterior abnormalities with slow performance on the 9-hole peg test. In conclusion, abnormalities in the corpus callosum can be assessed with quantitative MRI and are associated with cognitive and complex upper-extremity dysfunction in MS.
Figures

Similar articles
-
Segmented corpus callosum diffusivity correlates with the Expanded Disability Status Scale score in the early stages of relapsing-remitting multiple sclerosis.Clinics (Sao Paulo). 2013;68(8):1115-20. doi: 10.6061/clinics/2013(08)09. Clinics (Sao Paulo). 2013. PMID: 24037007 Free PMC article.
-
'Importance sampling' in MS: use of diffusion tensor tractography to quantify pathology related to specific impairment.J Neurol Sci. 2005 Oct 15;237(1-2):13-9. doi: 10.1016/j.jns.2005.04.019. J Neurol Sci. 2005. PMID: 16109428 Clinical Trial.
-
Influence of corpus callosum damage on cognition and physical disability in multiple sclerosis: a multimodal study.PLoS One. 2012;7(5):e37167. doi: 10.1371/journal.pone.0037167. Epub 2012 May 14. PLoS One. 2012. PMID: 22606347 Free PMC article.
-
The multiple sclerosis functional composite: a clinically meaningful measure of disability.Neurology. 2010 Apr 27;74 Suppl 3:S8-15. doi: 10.1212/WNL.0b013e3181dbb571. Neurology. 2010. PMID: 20421572 Review.
-
Corpus callosum damage to account for cognitive, affective, and social-cognitive dysfunctions in multiple sclerosis: A model of callosal disconnection syndrome?Mult Scler. 2023 Feb;29(2):160-168. doi: 10.1177/13524585221091067. Epub 2022 Apr 27. Mult Scler. 2023. PMID: 35475386 Review.
Cited by
-
Bayesian scalar-on-image regression with application to association between intracranial DTI and cognitive outcomes.Neuroimage. 2013 Dec;83:210-23. doi: 10.1016/j.neuroimage.2013.06.020. Epub 2013 Jun 17. Neuroimage. 2013. PMID: 23792220 Free PMC article.
-
White matter correlates of slowed information processing speed in unimpaired multiple sclerosis patients with young age onset.Brain Imaging Behav. 2021 Jun;15(3):1460-1468. doi: 10.1007/s11682-020-00345-z. Brain Imaging Behav. 2021. PMID: 32748319
-
Oestrogen receptor beta ligand: a novel treatment to enhance endogenous functional remyelination.Brain. 2010 Oct;133(10):2999-3016. doi: 10.1093/brain/awq237. Epub 2010 Sep 21. Brain. 2010. PMID: 20858739 Free PMC article.
-
Segmented corpus callosum diffusivity correlates with the Expanded Disability Status Scale score in the early stages of relapsing-remitting multiple sclerosis.Clinics (Sao Paulo). 2013;68(8):1115-20. doi: 10.6061/clinics/2013(08)09. Clinics (Sao Paulo). 2013. PMID: 24037007 Free PMC article.
-
Depressive symptoms, anxiety and cognitive impairment: emerging evidence in multiple sclerosis.Transl Psychiatry. 2023 Jul 19;13(1):264. doi: 10.1038/s41398-023-02555-7. Transl Psychiatry. 2023. PMID: 37468462 Free PMC article. Review.
References
-
- Gazzaniga MS. Cerebral specialization and interhemispheric communication: does the corpus callosum enable the human condition? Brain. 2000;123 ( Pt 7):1293–326. - PubMed
-
- Evangelou N, Konz D, Esiri MM, Smith S, Palace J, Matthews PM. Regional axonal loss in the corpus callosum correlates with cerebral white matter lesion volume and distribution in multiple sclerosis. Brain. 2000;123 ( Pt 9):1845–9. - PubMed
-
- Larson EB, Burnison DS, Brown WS. Callosal function in multiple sclerosis: bimanual motor coordination. Cortex. 2002;38:201–14. - PubMed
-
- Bobholz JA, Rao SM. Cognitive dysfunction in multiple sclerosis: a review of recent developments. Curr Opin Neurol. 2003;16:283–8. - PubMed
-
- Gronwall DM. Paced auditory serial-addition task: a measure of recovery from concussion. Percept Mot Skills. 1977;44:367–73. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
