

Intracerebral and subarachnoid hemorrhage in patients with cancer
- PMID: 20142616
- PMCID: PMC2830918
- DOI: 10.1212/WNL.0b013e3181cef837
Intracerebral and subarachnoid hemorrhage in patients with cancer
Abstract
Objective: To analyze the risk factors, presentation, etiologies, and outcomes of adult cancer patients with intracranial hemorrhage (IH).
Methods: We analyzed 208 patients retrospectively with the diagnosis of IH from the Memorial Sloan-Kettering neurology database from January 2000 through December 2007. Charts were examined for clinical and radiographic data. Survival was calculated using the Kaplan-Meier method. Survival between groups was compared via the log-rank test. Logistic regression models were used to assess for prognostic indicators of 30- and 90-day mortality.
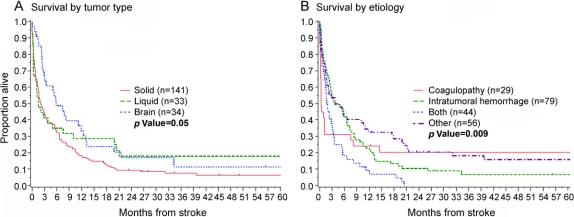
Results: There were 181 intracerebral and 46 subarachnoid hemorrhages. Sixty-eight percent of patients had solid tumors, 16% had primary brain tumors, and 16% had hematopoietic tumors. Hemiparesis and headache were the most common symptoms. Intratumoral hemorrhage (61%) and coagulopathy (46%) accounted for the majority of hemorrhages, whereas hypertension (5%) was rare. Median survival was 3 months (95% confidence interval [CI] 2-4), and 30-day mortality was 31%. However, nearly one-half of patients were completely or partially independent at the time of discharge. Patients with primary brain tumors had the longest median survival (5.9 months, 95% CI 2.9-11.8, p = 0.05). Independent predictors of 30-day mortality were not having a primary brain tumor, impaired consciousness, multiple foci of hemorrhage, hydrocephalus, no ventriculostomy, and treatment of increased intracranial pressure.
Conclusions: Intracranial hemorrhage in patients with cancer is often due to unique mechanisms. Prognosis is poor, but comparable to intracranial hemorrhage in the general population. Aggressive care is recommended despite high mortality, because many patients have good functional outcomes.
Figures
References
-
- Graus F, Rogers LR, Posner JB. Cerebrovascular complications in patients with cancer. Medicine 1985;64:16–35. - PubMed
-
- Jellinger K. Pathology of intracerebral hemorrhage. Zentralbl Neurochir 1977;38:29–42. - PubMed
-
- Yamauchi K, Umeda Y. Symptomatic intracranial haemorrhage in acute nonlymphoblastic leukaemia: analysis of CT and autopsy findings. J Neurol 1997;244:94–100. - PubMed
-
- Padt JP, De Reuck J, Eecken HV. Intracerebral hemorrhage as initial symptom of a brain tumor. Acta Neurol Belg 1973;73:241–251. - PubMed
-
- Gildersleeve N, Koo AH, McDonald CJ. Metastatic tumor presenting as intracerebral hemorrhage. Radiology 1977;124:109–112. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources