

Involvement of lymphatics in lymphangioleiomyomatosis
- PMID: 20143921
- PMCID: PMC2883505
- DOI: 10.1089/lrb.2009.0017
Involvement of lymphatics in lymphangioleiomyomatosis
Abstract
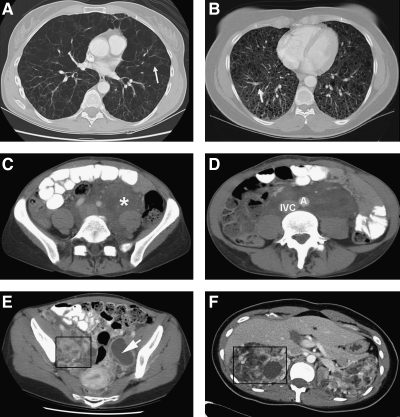
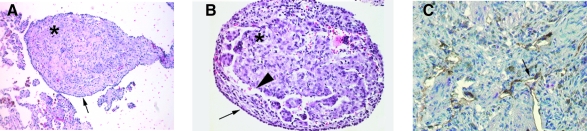
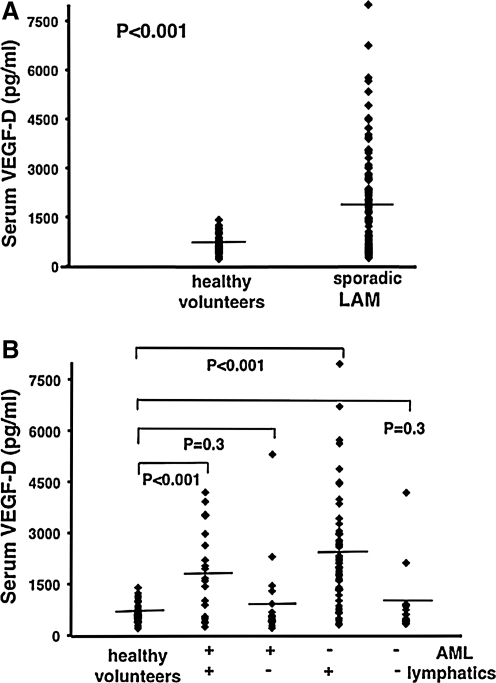
Lymphangioleiomyomatosis (LAM), a rare multisystem disease, occurs primarily in women, with cystic destruction of the lungs, abdominal tumors, and involvement of the axial lymphatics in the thorax and abdomen. To understand the pathogenesis of LAM, we initiated a longitudinal study of patients with LAM; over 500 patients have been enrolled. LAM results from the proliferation of a neoplastic cell (LAM cell), which has mutations in the tuberous sclerosis complex (TSC) genes, TSC1 or TSC2. Consistent with their metastatic behavior, LAM cells were isolated from blood, urine, and chylous effusions. Surface proteins on LAM cells include those found on metastatic cells and those involved in cell migration. In the lung, LAM cells are found clustered in nodules, which appear in the walls of the cysts, and in the interstitium. LAM lung nodules are traversed by slit-like vascular structures, with lining cells showing reactivity with antibodies against components of lymphatic endothelial cells. The axial lymphatics appear to be infiltrated by LAM cells, which may result in obstruction and formation of chyle-filled lymphangioleiomyomas. LAM cell clusters have been isolated from chylous pleural effusions, and it is hypothesized that these clusters may be responsible for metastatic spread of LAM cells via lymphatic vessels. Consistent with a lymphangiogenic process, levels of VEGF-D, a lymphangiogenic factor, were higher in sera of patients with LAM and lymphatic involvement (i.e., lymphangioleiomyoma, adenopathy) than in healthy volunteers or LAM patients with cystic disease limited to the lung. These findings are consistent with an important function for lymphangiogenesis in LAM.
Figures
Similar articles
-
Lymphatic involvement in lymphangioleiomyomatosis.Ann N Y Acad Sci. 2008;1131:206-14. doi: 10.1196/annals.1413.018. Ann N Y Acad Sci. 2008. PMID: 18519973 Free PMC article. Review.
-
Serum vascular endothelial growth factor-D levels in patients with lymphangioleiomyomatosis reflect lymphatic involvement.Chest. 2009 May;135(5):1293-1300. doi: 10.1378/chest.08-1160. Chest. 2009. PMID: 19420197 Free PMC article.
-
Lymphatics in lymphangioleiomyomatosis and idiopathic pulmonary fibrosis.Eur Respir Rev. 2012 Sep 1;21(125):196-206. doi: 10.1183/09059180.00009311. Eur Respir Rev. 2012. PMID: 22941884 Free PMC article. Review.
-
Diagnostic and Treatment Monitoring Potential of Serum Vascular Endothelial Growth Factor-D in Lymphangioleiomyomatosis.Lymphology. 2016 Sep;49(3):140-9. Lymphology. 2016. PMID: 29906075
-
Sirolimus decreases circulating lymphangioleiomyomatosis cells in patients with lymphangioleiomyomatosis.Chest. 2014 Jan;145(1):108-112. doi: 10.1378/chest.13-1071. Chest. 2014. PMID: 24051985 Free PMC article.
Cited by
-
A pulmonary lymphangioleiomyomatosis with multi-site angiomyolipoma: a case report.Transl Cancer Res. 2022 Jul;11(7):2449-2456. doi: 10.21037/tcr-21-2539. Transl Cancer Res. 2022. PMID: 35966317 Free PMC article.
-
Targeting Fibroblast-Endothelial Interactions in LAM Pathogenesis: 3D Spheroid and Spatial Transcriptomic Insights for Therapeutic Innovation.bioRxiv [Preprint]. 2024 Sep 6:2023.06.12.544372. doi: 10.1101/2023.06.12.544372. bioRxiv. 2024. Update in: JCI Insight. 2025 Feb 04;10(6):e187899. doi: 10.1172/jci.insight.187899. PMID: 37398026 Free PMC article. Updated. Preprint.
-
Low-dose sirolimus in retroperitoneal lymphangioleiomyomas.Lung India. 2019 Jul-Aug;36(4):349-352. doi: 10.4103/lungindia.lungindia_433_18. Lung India. 2019. PMID: 31290423 Free PMC article.
-
Changes in lung function and chylous effusions in patients with lymphangioleiomyomatosis treated with sirolimus.Ann Intern Med. 2011 Jun 21;154(12):797-805, W-292-3. doi: 10.7326/0003-4819-154-12-201106210-00007. Ann Intern Med. 2011. PMID: 21690594 Free PMC article.
-
Cervical Lymphangiolipoleiomyoma: An Unusual Offender at a Usual Destination - Case Report and Literature Review.J Midlife Health. 2025 Apr-Jun;16(2):211-214. doi: 10.4103/jmh.jmh_4_25. Epub 2025 May 6. J Midlife Health. 2025. PMID: 40636839 Free PMC article.
References
-
- Kitaichi M. Nishimura K. Itoh H. Izumi T. Pulmonary lymphangioleiomyomatosis: A report of patients including a clinicopathologic study of prognostic factors. Am J Respir Crit Care Med. 1995;151:527–533. - PubMed
-
- Chu S. Horiba K. Usuki J. Avila N. Chen C. Travis W. Ferrans V. Moss J. Comprehensive evaluation of 35 patients with lymphangioleiomyomatosis. Chest. 1999;115:1041–1052. - PubMed
-
- Urban T. Lazor R. Lacronique J. Murris M. Labrune S. Valeyre D. Cordier J–F. Pulmonary lymphangioleiomyomatosis: A study of 69 patients. Medicine. 1999;78:321–337. - PubMed
-
- Ryu J. Moss J. Beck G. Lee J–C. Brown K. Chapman J. Finlay G. Olson E. Ross S. Maurer J. Raffin T. Peavy H. McCarthy K. Taveira–DaSilva A. McCormack F. Avila N. DeCastro R. Jacobs S. Stylianou M. Fanburg B for the NHLBI LAM Registry Group. The NHLBI lymphangioleiomyomatosis registry: Characteristics of 230 patients at enrollment. Am J Respir Crit Care Med. 2006;173:105–111. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
