

Epidemiological profile of meningococcal disease in the United States
- PMID: 20144015
- PMCID: PMC2820831
- DOI: 10.1086/648963
Epidemiological profile of meningococcal disease in the United States
Abstract
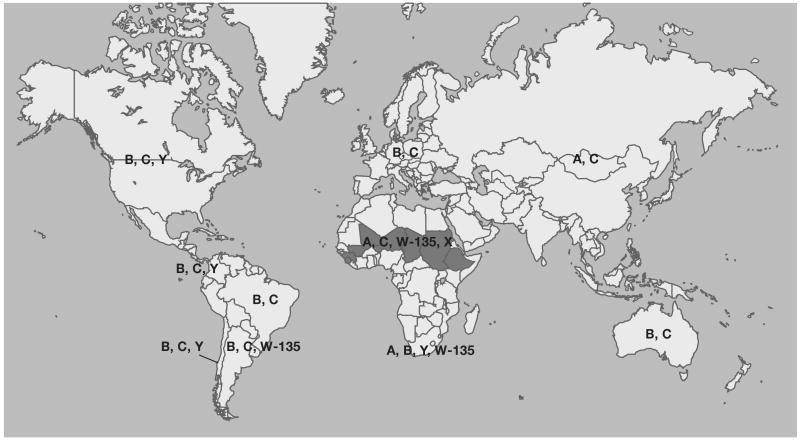
Neisseria meningitidis is a leading cause of bacterial meningitis and other serious infections worldwide. The epidemiological profile of N. meningitidis is highly changeable, with great differences in disease incidence and serogroup distribution. Six serogroups (namely serogroups A, B, C, W-135, X, and Y) are responsible for most cases of meningococcal disease worldwide; the epidemiological profile of disease caused by each serogroup is unique. No vaccine is available for endemic disease caused by serogroup B strains. Two tetravalent (A/C/Y/W-135) meningococcal vaccines are licensed in the United States: a purified polysaccharide product and a polysaccharide-protein conjugate vaccine. The conjugate vaccine is recommended for all adolescents, although vaccine coverage remains low, and other groups at high risk of infection. A comprehensive program to prevent invasive meningococcal disease in the United States will require vaccination of infants; several conjugate vaccines for infants may become available in the near future. Broadly protective vaccines for endemic serogroup B disease are also needed.
Figures
References
-
- Harrison LH, Trotter CL, Ramsay ME. Global epidemiology of meningococcal disease. Vaccine. 2009;27 2:B51–63. - PubMed
-
- Granoff DM, Harrison LH, Borrow R. Meningococcal vaccines. In: Plotkin S, Orenstein WA, Offit PA, editors. Vaccines. Fifth. Philadelphia: Saunders Elsevier; 2008. pp. 399–434.
-
- Harrison LH, Broome CV. The epidemiology of meningococcal meningitis in the U.S civilian population. In: Vedros NA, editor. Evolution of meningococcal disease. Vol. 1. Boca Raton, Fla: CRC Press; 1987. pp. 27–45.
