

Oral insulin and buccal insulin: a critical reappraisal
- PMID: 20144297
- PMCID: PMC2769877
- DOI: 10.1177/193229680900300323
Oral insulin and buccal insulin: a critical reappraisal
Abstract
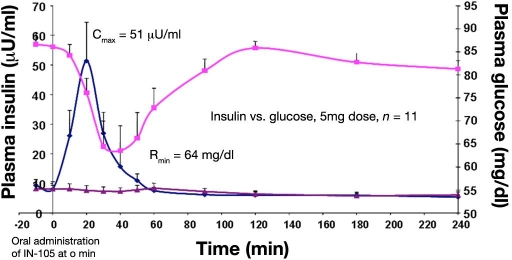
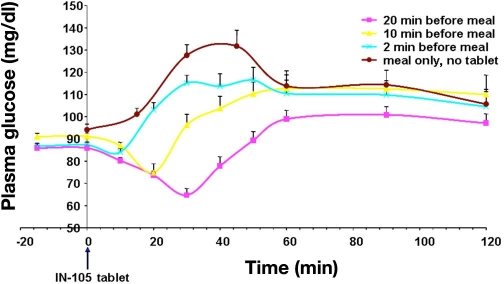
Despite the availability of modern insulin injection devices with needles that are so sharp and thin that practically no injection pain takes place, it is still the dream of patients with diabetes to, for example, swallow a tablet with insulin. This is not associated with any pain and would allow more discretion. Therefore, availability of oral insulin would not only ease insulin therapy, it would certainly increase compliance. However, despite numerous attempts to develop such a "tablet" in the past 85 years, still no oral insulin is commercially available. Buccal insulin is currently in the last stages of clinical development by one company and might become available in the United States and Europe in the coming years (it is already on the market in some other countries). The aim of this review is to critically describe the different approaches that are currently under development. Optimal coverage of prandial insulin requirements is the aim with both routes of insulin administration (at least with most approaches). The speed of onset of metabolic effect seen with some oral insulin approaches is rapid, but absorption appears to be lower when the tablet is taken immediately prior to a meal. With all approaches, considerable amounts of insulin have to be applied in order to induce therapeutically relevant increases in the metabolic effect because of the low relative biopotency of buccal insulin. Unfortunately, the number of publications about clinical-experimental and clinical studies is surprisingly low. In addition, there is no study published in which the variability of the metabolic effect induced (with and without a meal) was studied adequately. In summary, after the failure of inhaled insulin, oral insulin and buccal insulin are hot candidates to come to the market as the next alternative routes of insulin administration.
2009 Diabetes Technology Society.
Figures
References
-
- Pettis RJ, Hompesch M, Kapitza C, Harvey NG, Ginsberg B, Heinemann L. Intra-dermal insulin lispro application with a new microneedle delivery system led to a substantially more rapid insulin absorption than subcutaneous injection. Diabetes. 2006;55(Suppl 1):A26.
-
- Carino GP, Mathiowitz E. Oral insulin delivery. Adv Drug Deliv Rev. 1999;35(2-3):249–257. - PubMed
-
- Lassmann-Vague V, Raccah D. Alternative routes of insulin delivery. Diabetes Metab. 2006;32(5 Pt 2):513–522. - PubMed
-
- Owens DR, Zinman B, Bolli G. Alternative routes of insulin delivery. Diabet Med. 2003;20(11):886–898. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
