

Reducing glycemic variability in intensive care unit patients: a new therapeutic target?
- PMID: 20144384
- PMCID: PMC2787030
- DOI: 10.1177/193229680900300610
Reducing glycemic variability in intensive care unit patients: a new therapeutic target?
Abstract
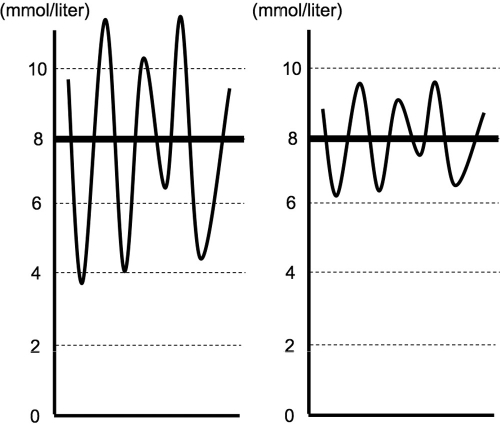
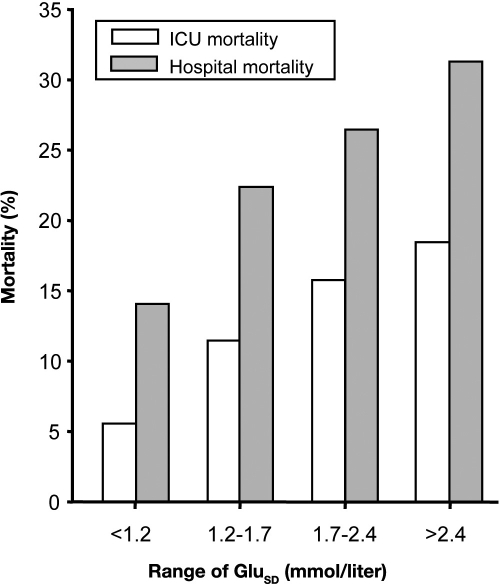
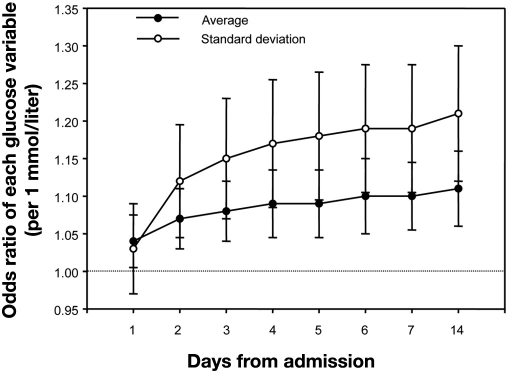
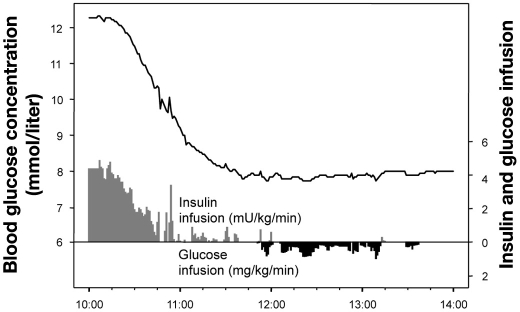
Acute hyperglycemia is common in critically ill patients. Strict control of blood glucose (BG) concentration has been considered important because hyperglycemia is associated independently with increased intensive care unit mortality. After intensive insulin therapy was reported to reduce mortality in selected surgical critically ill patients, lowering of BG levels was recommended as a means of improving patient outcomes. However, a large multicenter multination study has found that intensive insulin therapy increased mortality significantly. A difference in variability of BG control may be one possible explanation why the effect of intensive insulin therapy varied from beneficial to harmful. Several studies have confirmed significant associations between variability of BG levels and patient outcomes. Decreasing the variability of the BG concentration may be an important dimension of glucose management. If reducing swings in the BG concentration is a major biologic mechanism behind the putative benefits of glucose control, it may not be necessary to pursue lower glucose levels with their attendant risk of hypoglycemia.
Figures
Similar articles
-
Glycemic control in the medical intensive care unit.J Diabetes Sci Technol. 2009 Nov 1;3(6):1330-41. doi: 10.1177/193229680900300613. J Diabetes Sci Technol. 2009. PMID: 20144387 Free PMC article. Review.
-
Blood glucose control in the trauma patient.J Diabetes Sci Technol. 2009 Nov 1;3(6):1373-6. doi: 10.1177/193229680900300617. J Diabetes Sci Technol. 2009. PMID: 20144391 Free PMC article. Review.
-
Risk of Hypoglycemia During Insulin Infusion Directed by Paper Protocol Versus Electronic Glycemic Management System in Critically Ill Patients at a Large Academic Medical Center.J Diabetes Sci Technol. 2018 Jan;12(1):47-52. doi: 10.1177/1932296817747617. Epub 2017 Dec 17. J Diabetes Sci Technol. 2018. PMID: 29251064 Free PMC article.
-
Perioperative and critical illness dysglycemia--controlling the iceberg.J Diabetes Sci Technol. 2009 Nov 1;3(6):1288-91. doi: 10.1177/193229680900300608. J Diabetes Sci Technol. 2009. PMID: 20144382 Free PMC article. Review.
-
Blood glucose controller for neonatal intensive care: virtual trials development and first clinical trials.J Diabetes Sci Technol. 2009 Sep 1;3(5):1066-81. doi: 10.1177/193229680900300510. J Diabetes Sci Technol. 2009. PMID: 20144420 Free PMC article. Clinical Trial.
Cited by
-
Risk-Based Care: Let's Think Outside the Box.Front Med (Lausanne). 2021 Feb 25;8:535244. doi: 10.3389/fmed.2021.535244. eCollection 2021. Front Med (Lausanne). 2021. PMID: 33718394 Free PMC article. No abstract available.
-
Increasing blood glucose variability heralds hypoglycemia in the critically ill.J Surg Res. 2011 Oct;170(2):257-64. doi: 10.1016/j.jss.2011.03.008. Epub 2011 Mar 31. J Surg Res. 2011. PMID: 21543086 Free PMC article.
-
Estimating Enhanced Endogenous Glucose Production in Intensive Care Unit Patients with Severe Insulin Resistance.J Diabetes Sci Technol. 2022 Sep;16(5):1208-1219. doi: 10.1177/19322968211018260. Epub 2021 Jun 2. J Diabetes Sci Technol. 2022. PMID: 34078114 Free PMC article.
-
Changes in blood glucose of elderly patients with gastric cancer combined with type 2 diabetes mellitus after radical operation and the effect of mediation adjustment for blood glucose on the recovery of gastric cancer.Oncol Lett. 2018 Oct;16(4):4303-4308. doi: 10.3892/ol.2018.9197. Epub 2018 Jul 23. Oncol Lett. 2018. PMID: 30214565 Free PMC article.
-
Glycemic variability and mortality in oncologic intensive care units.Rev Bras Enferm. 2023 Oct 9;76(4):e20220812. doi: 10.1590/0034-7167-2022-0812. eCollection 2023. Rev Bras Enferm. 2023. PMID: 37820156 Free PMC article.
References
-
- Wolfe RR, Allsop JR, Burke JF. Glucose metabolism in man: responses to intravenous glucose infusion. Metabolism. 1979;28(3):210–220. - PubMed
-
- Shangraw RE, Jahoor F, Miyoshi H, Neff WA, Stuart CA, Herndon DN, Wolfe RR. Differentiation between septic and postburn insulin resistance. Metabolism. 1989;38(10):983–989. - PubMed
-
- Cely CM, Arora P, Quartin AA, Kett DH, Schein RM. Relationship of baseline glucose homeostasis to hyperglycemia during medical critical illness. Chest. 2004;126(3):879–887. - PubMed
-
- McCowen KC, Malhotra A, Bistrian BR. Stress-induced hyperglycemia. Crit Care Clin. 2001;17(1):107–124. - PubMed
-
- Van den Berghe G, Wouters P, Weekers F, Verwaest C, Bruyninckx F, Schetz M, Vlasselaers D, Ferdinande P, Lauwers P, Bouillon R. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345(19):1359–1367. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
