

Review
doi: 10.1177/193229680900300611.
Clinical need for continuous glucose monitoring in the hospital
Affiliations
- PMID: 20144385
- PMCID: PMC2787031
- DOI: 10.1177/193229680900300611
Item in Clipboard
Review
Clinical need for continuous glucose monitoring in the hospital
J Diabetes Sci Technol.
.
Abstract
Automation and standardization of the glucose measurement process have the potential to greatly improve glycemic control, clinical outcome, and safety while reducing cost. The resources required to monitor glycemia in hospitalized patients have thus far limited the implementation of intensive glucose management to patients in critical care units. Numerous available and up-and-coming technologies are targeted for the hospital patient population. Advantages and limitations of these devices are discussed herewith in.
Figures
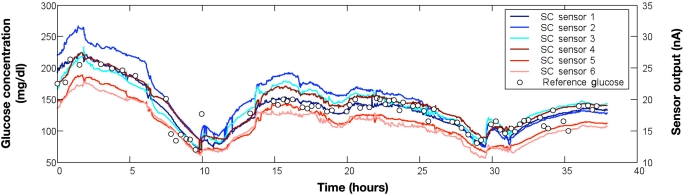
Glucose trend data measured simultaneously from six interstitial fluid continuous glucose monitors (modified research-only Guardian RT systems, Medtronic Diabetes, Northridge, CA) during and after major abdominal surgery. Patient had type 2 diabetes managed chronically with subcutaneous insulin and managed currently with an intravenous infusion of regular insulin. All CGM measurements moved in parallel (direction and rate of change) during the 38 hours of data collection. Several CGM sensors correlated closely with reference blood glucose measurements (blood sampled from a radial artery catheter and measured in duplicate using an Omni-9 analyzer; Roche Diagnostics). Several CGM sensors, however, demonstrated a consistent negative or positive bias relative to the reference BG measurements.

A continuous glucose monitor was inserted into the thigh of a hospitalized patient with type 2 diabetes managed with subcutaneous insulin. A CGMS iPro Recorder (Medtronic Diabetes, Northridge, CA) measured and recorded the concentration of interstitial fluid glucose every 5 minutes. Sensor output current (thin line) was calibrated to POC measurements from an Accu-Chek Inform meter (solid circles) and the hospital laboratory (solid squares) to produce an estimate of blood glucose (thick line). Recurrent hypoglycemia was recorded twice over the 72-hour study period.
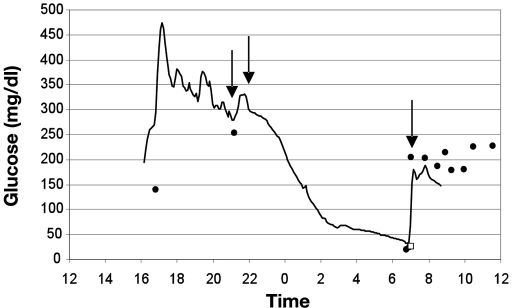
Severe hypoglycemia recorded in a hospitalized patient with type 1 diabetes 1 day after orthopedic surgery. The interstitial fluid glucose concentration (solid line) was measured and recorded every 5 minutes using a CGMS iPro Continuous Glucose Recorder (Medtronic Diabetes, Northridge, CA). CGM data were calibrated using a retrospective method using POC glucose measurements (solid circles) from an Accu-Chek Inform meter (Roche Diagnostics USA, Indianapolis, IN), thus the clinical nurse was blinded to real-time CGM data. Capillary BG measurements at 1700 and 2100 hours were elevated. Peakless and rapid-acting insulin were injected into the subcutaneous tissue around 2100 hours. The patient was found unresponsive at 0700 hours with a POC glucose of 18 mg/dl and a central laboratory plasma glucose of 26 mg/dl (open square). A bolus dose of 50% glucose (25 grams) was delivered into the IV catheter at 0710 hours. The patient recovered without permanent injury. This adverse event could have been prevented if the nurse had access to real-time CGM data.
References
-
- Krinsley JS. Association between hyperglycemia and increased hospital mortality in a heterogeneous population of critically ill patients. Mayo Clin Proc. 2003;78(12):1471–1478. - PubMed
-
- Krinsley JS, Grover A. Severe hypoglycemia in critically ill patients: risk factors and outcomes. Crit Care Med. 2007;35(10):2262–2267. - PubMed
-
- Clement S, Braithwaite SS, Magee MF, Ahmann A, Smith EP, Schafer RG, Hirsch IB American Diabetes Association Diabetes in Hospitals Writing Committee. Management of diabetes and hyperglycemia in hospitals. Diabetes Care. 2004;27(2):553–591. - PubMed
-
- Cryer PE. Hypoglycaemia: the limiting factor in the glycaemic management of the critically ill? Diabetologia. 2006;49(8):1722–1725. - PubMed
-
- Braithwaite SS, Buie MM, Thompson CL, Baldwin DF, Oertel MD, Robertson BA, Mehrotra HP. Hospital hypoglycemia: not only treatment but also prevention. Endocr Pract. 2004;10(Suppl 2):89–99. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
