

Glycemic control in the medical intensive care unit
- PMID: 20144387
- PMCID: PMC2787033
- DOI: 10.1177/193229680900300613
Glycemic control in the medical intensive care unit
Abstract
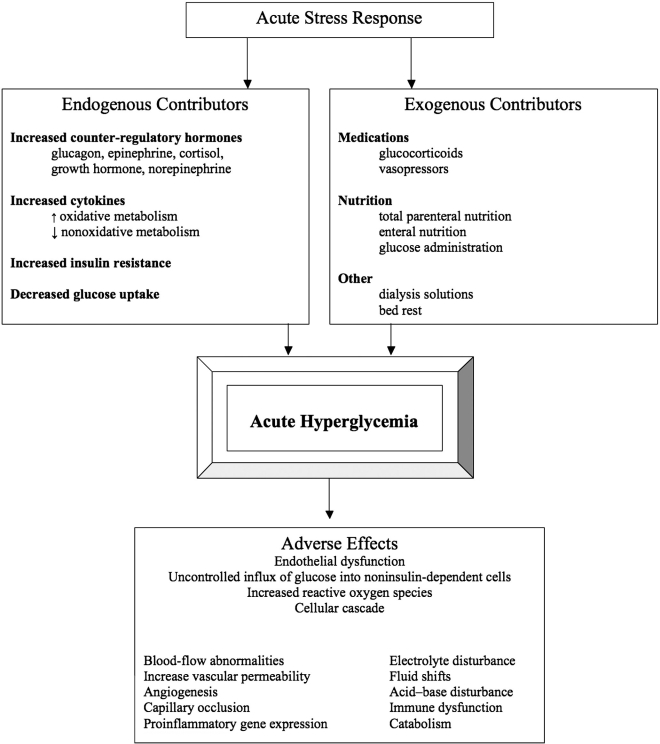
Hyperglycemia in the critically ill is a well-known phenomenon, even in those without known diabetes. The stress response is due to a complex interplay between counter-regulatory hormones, cytokines, and changes in insulin sensitivity. Illness/infection, overfeeding, medications (e.g., corticosteroids), insufficient insulin, and/or volume depletion can be additional contributors. Acute hyperglycemia can adversely affect fluid balance (through glycosuria and dehydration), immune and endothelial function, inflammation, and outcome. While there are several insulin infusion protocols that are able to safely and effectively treat hyperglycemia, the bulk of accumulated evidence does not support a causal relationship between acute hyperglycemia and adverse outcomes in the medical intensive care unit. Meta-analysis of randomized controlled trials suggests there is no benefit to tightening glucose control to normal levels compared to a reasonable and achievable goal of 140 to 180 mg/dl. There is a significantly increased risk of hypoglycemia. Although there is some evidence that patients without known diabetes have worse outcomes than those with known diabetes, more recent evidence is conflicting. Glycemic control in critically ill patients should not be neglected, as studies have not tested tight versus no/poor control, but tight versus good control. A moderate approach to managing critical illness hyperglycemia seems most prudent at this juncture. Future research should ascertain whether there are certain subgroups of patients that would benefit from tighter glycemic goals. It also remains to be seen if tight glucose control is beneficial once hypoglycemia is minimized with technological advances such as continuous glucose monitoring systems.
Figures
Similar articles
-
Perioperative and critical illness dysglycemia--controlling the iceberg.J Diabetes Sci Technol. 2009 Nov 1;3(6):1288-91. doi: 10.1177/193229680900300608. J Diabetes Sci Technol. 2009. PMID: 20144382 Free PMC article. Review.
-
Blood glucose control in the trauma patient.J Diabetes Sci Technol. 2009 Nov 1;3(6):1373-6. doi: 10.1177/193229680900300617. J Diabetes Sci Technol. 2009. PMID: 20144391 Free PMC article. Review.
-
An overview of glycemic control in the coronary care unit with recommendations for clinical management.J Diabetes Sci Technol. 2009 Nov 1;3(6):1342-51. doi: 10.1177/193229680900300614. J Diabetes Sci Technol. 2009. PMID: 20144388 Free PMC article. Review.
-
Glucose control in the intensive care unit.Crit Care Med. 2009 May;37(5):1769-76. doi: 10.1097/CCM.0b013e3181a19ceb. Crit Care Med. 2009. PMID: 19325461 Review.
-
Reducing glycemic variability in intensive care unit patients: a new therapeutic target?J Diabetes Sci Technol. 2009 Nov 1;3(6):1302-8. doi: 10.1177/193229680900300610. J Diabetes Sci Technol. 2009. PMID: 20144384 Free PMC article. Review.
Cited by
-
Diabetes aggravates acute pancreatitis and inhibits pancreas regeneration in mice.Diabetologia. 2012 May;55(5):1526-34. doi: 10.1007/s00125-012-2479-3. Epub 2012 Feb 12. Diabetologia. 2012. PMID: 22327285
-
Tight glycemic control in critically ill pediatric patients: a systematic review and meta-analysis.Crit Care. 2018 Mar 4;22(1):57. doi: 10.1186/s13054-018-1976-2. Crit Care. 2018. PMID: 29501063 Free PMC article.
-
Liraglutide as an Alternative to Insulin for Glycemic Control in Intensive Care Unit: A Randomized, Open-label, Clinical Study.Indian J Crit Care Med. 2017 Sep;21(9):568-572. doi: 10.4103/ijccm.IJCCM_105_17. Indian J Crit Care Med. 2017. PMID: 28970655 Free PMC article.
-
Tight glycemic control and cardiovascular effects in type 2 diabetic patients.Heart Views. 2014 Oct-Dec;15(4):111-20. doi: 10.4103/1995-705X.151084. Heart Views. 2014. PMID: 25774253 Free PMC article. Review.
-
Glycemic control in critically ill patients.World J Crit Care Med. 2012 Feb 4;1(1):31-9. doi: 10.5492/wjccm.v1.i1.31. eCollection 2012 Feb 4. World J Crit Care Med. 2012. PMID: 24701399 Free PMC article. Review.
References
-
- Van den Berghe G, Wouters P, Weekers F, Verwaest C, Bruyninckx F, Schetz M, Vlasselaers D, Ferdinande P, Lauwers P, Bouillon R. Intensive insulin therapy in the critically ill patients. New Engl J Med. 2001;345(19):1359–1367. - PubMed
-
- Cely CM, Arora P, Quartin AA, Kett DH, Schein RM. Relationship of baseline glucose homeostasis to hyperglycemia during medical critical illness. Chest. 2004;126(3):879–887. - PubMed
-
- Gandhi GY, Nuttall GA, Abel MD, Mullany CJ, Schaff HV, O'Brien PC, Johnson MG, Williams AR, Cutshall SM, Mundy LM, Rizza RA, McMahon MM. Intensive intraoperative insulin therapy versus conventional glucose management during cardiac surgery: a randomized trial. Ann Intern Med. 2007;146(4):233–243. - PubMed
-
- Blumberg D, Hochwald S, Burt M, Donner D, Brennan MF. Tumor necrosis factor alpha stimulates gluconeogenesis from alanine in vivo. J Surg Oncol. 1995;59(4):220–224. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
