

Reducing cardiometabolic risk in peritoneal dialysis patients: role of the dialysis solution
- PMID: 20144403
- PMCID: PMC2787049
- DOI: 10.1177/193229680900300629
Reducing cardiometabolic risk in peritoneal dialysis patients: role of the dialysis solution
Abstract
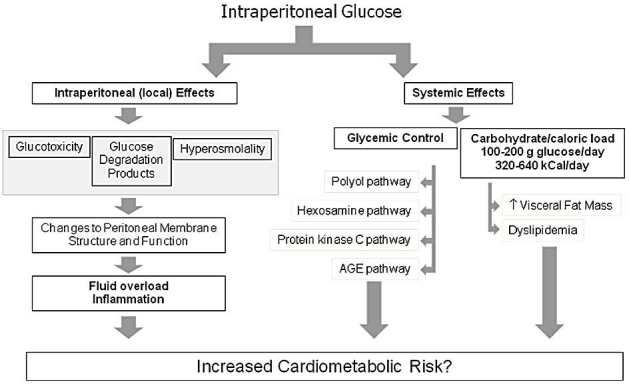
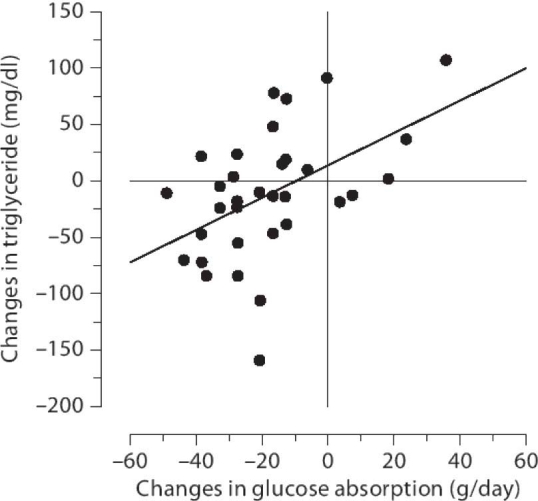
Peritoneal dialysis (PD) is a well-established form of therapy for stage 5 chronic kidney disease requiring renal replacement therapy. D-Glucose has been used successfully for several decades as the osmotic agent employed in dialysis solutions to achieve adequate fluid removal. The absorption of 100-200 grams of glucose per day has been suggested as potentially increasing cardiometabolic risk, particularly in patients with diabetes. Supporting and undermining evidence for this hypothesis is reviewed, with a focus on the role of glucose absorption in changes in body composition, dyslipidemia, and glycemic control in diabetic PD patients. Clinical strategies to optimize fluid removal while minimizing the metabolic impact of glucose absorption are also discussed.
Figures
Similar articles
-
Adverse effects of systemic glucose absorption with peritoneal dialysis: how good is the evidence?Curr Opin Nephrol Hypertens. 2013 Nov;22(6):663-8. doi: 10.1097/MNH.0b013e328365b3d1. Curr Opin Nephrol Hypertens. 2013. PMID: 24076559 Review.
-
Insulin resistance and glucose homeostasis in peritoneal dialysis.Perit Dial Int. 2009 Feb;29 Suppl 2:S145-8. Perit Dial Int. 2009. PMID: 19270204 Review.
-
Peritoneal dialysis in diabetic patients.Contrib Nephrol. 2001;(131):51-60. doi: 10.1159/000060060. Contrib Nephrol. 2001. PMID: 11125563 Review. No abstract available.
-
Biocompatible peritoneal dialysis solutions: do we have one?Clin J Am Soc Nephrol. 2010 Apr;5(4):723-32. doi: 10.2215/CJN.05720809. Epub 2010 Jan 21. Clin J Am Soc Nephrol. 2010. PMID: 20093342 Review.
-
Treatment targets for diabetic patients on peritoneal dialysis: any evidence?Perit Dial Int. 2007 Jun;27 Suppl 2:S176-9. Perit Dial Int. 2007. PMID: 17556300 Review.
Cited by
-
Association between Dyslipidemia and Peritoneal Dialysis Technique Survival.Open Access Maced J Med Sci. 2019 Jul 25;7(15):2467-2473. doi: 10.3889/oamjms.2019.664. eCollection 2019 Aug 15. Open Access Maced J Med Sci. 2019. PMID: 31666849 Free PMC article.
-
Hyperbranched polyglycerol is superior to glucose for long-term preservation of peritoneal membrane in a rat model of chronic peritoneal dialysis.J Transl Med. 2016 Dec 13;14(1):338. doi: 10.1186/s12967-016-1098-z. J Transl Med. 2016. PMID: 27964722 Free PMC article.
-
Peritoneal dialysis in diabetics: there is room for more.Int J Nephrol. 2011;2011:914849. doi: 10.4061/2011/914849. Epub 2011 Oct 16. Int J Nephrol. 2011. PMID: 22013524 Free PMC article.
-
Stability of the combination of ceftazidime and cephazolin in icodextrin or pH neutral peritoneal dialysis solution.Perit Dial Int. 2014 Mar-Apr;34(2):212-8. doi: 10.3747/pdi.2013.00034. Epub 2014 Jan 2. Perit Dial Int. 2014. PMID: 24385326 Free PMC article.
-
An update on peritoneal dialysis solutions.Nat Rev Nephrol. 2012 Feb 21;8(4):224-33. doi: 10.1038/nrneph.2012.13. Nat Rev Nephrol. 2012. PMID: 22349485 Review.
References
-
- United States Renal Data System. USRDS Coordinating Center. 2008. Available from: http://www.usrds.org.
-
- Holmes CJ. Glucotoxicity in peritoneal dialysis–solutions for the solution! Adv Chronic Kidney Dis. 2007;14(30):269–278. - PubMed
-
- Marshall J, Jennings P, Scott A, Fluck RJ, McIntyre CW. Glycemic control in diabetic CAPD patients assessed by continuous glucose monitoring system (CGMS) Kidney Int. 2003;64(4):1480–1486. - PubMed
-
- Hithaishi C, Lobbedez T, Padmanabhan S, Pineda ME, Oreopoulos DG. No beneficial effect of icodextrin on blood glucose control. Perit Dial Int. 2004;24(2):199–200. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
