

Phase I oncology studies: evidence that in the era of targeted therapies patients on lower doses do not fare worse
- PMID: 20145187
- PMCID: PMC2822881
- DOI: 10.1158/1078-0432.CCR-09-2684
Phase I oncology studies: evidence that in the era of targeted therapies patients on lower doses do not fare worse
Abstract
Purpose: To safely assess new drugs, cancer patients in initial cohorts of phase I oncology studies receive low drug doses. Doses are successively increased until the maximum tolerated dose (MTD) is determined. Because traditional chemotherapy is often more effective near the MTD, ethical concerns have been raised about administration of low drug doses to phase I patients. However, a substantial portion of oncology trials now investigate targeted agents, which may have different dose-response relationships than cytotoxic chemotherapies.
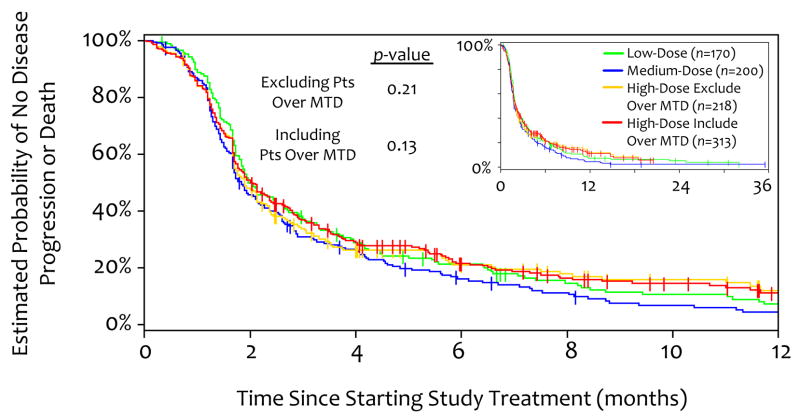
Experimental design: Twenty-four consecutive trials treating 683 patients between October 1, 2004, and June 30, 2008, at MD Anderson Cancer Center were analyzed. Patients were assigned to a low-dose (<or=25% MTD), medium-dose (25-75% MTD), or high-dose (>or=75% MTD) group, and groups were compared for response rate, time-to-treatment failure, progression-free survival, overall survival, and toxicity. To remove negatively biasing data from the high-dose group, in a second analysis, patients treated above the MTD were excluded (high-dose group, 75-100% MTD). Of the 683 patients, 97.7% received targeted agents.
Results: Even when excluding patients above the MTD, there was an early trend favoring the low- versus high-dose group in time-to-treatment failure, with 32.9% versus 25.2% of patients on therapy at 3 months (P = 0.08). In addition, the low-dose group fared at least as well as the other groups in all other outcomes, including response rate, progression-free survival, overall survival, and toxicity.
Conclusions: These data may help alleviate concerns that patients who receive low drug doses on contemporary phase I oncology trials fare worse and suggest targeted agents may have different dose-response relationships than cytotoxic chemotherapies.
Conflict of interest statement
None of the authors have any conflicts of interest relevant to the subject of this manuscript.
Figures



Comment in
-
Finding the right dose for cancer therapeutics--can we do better?Clin Cancer Res. 2010 Feb 15;16(4):1085-7. doi: 10.1158/1078-0432.CCR-09-3246. Epub 2010 Feb 9. Clin Cancer Res. 2010. PMID: 20145182
References
-
- Critical role of phase I clinical trials in cancer treatment. American Society of Clinical Oncology. J Clin Oncol. 1997;15:853–9. - PubMed
-
- Von Hoff DD, Turner J. Response rates, duration of response, and dose response effects in phase I studies of antineoplastics. Invest New Drugs. 1991;9:115–22. - PubMed
-
- Eisenhauer EA, O’Dwyer PJ, Christian M, Humphrey JS. Phase I clinical trial design in cancer drug development. J Clin Oncol. 2000;18:684–92. - PubMed
-
- Rogatko A, Babb JS, Tighiouart M, Khuri FR, Hudes G. New paradigm in dose-finding trials: patient-specific dosing and beyond phase I. Clin Cancer Res. 2005;11:5342–6. - PubMed
-
- Daugherty CK. Ethical issues in the development of new agents. Invest New Drugs. 1999;17:145–53. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
