

Limited-stage small cell lung cancer: current chemoradiotherapy treatment paradigms
- PMID: 20145192
- PMCID: PMC3227940
- DOI: 10.1634/theoncologist.2009-0298
Limited-stage small cell lung cancer: current chemoradiotherapy treatment paradigms
Abstract
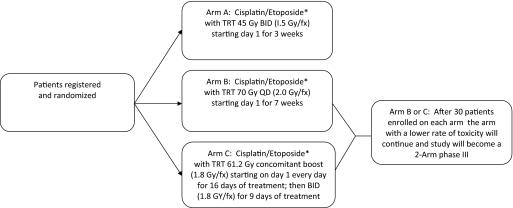
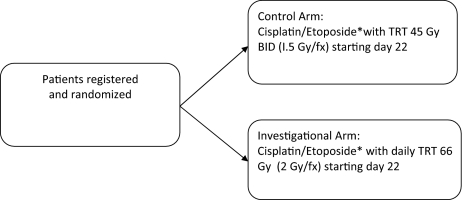
In the U.S., the prevalence of small cell lung cancer (SCLC) is declining, probably reflecting the decreasing prevalence of tobacco use. However, a significant number of patients will receive a diagnosis of SCLC, and approximately 40% of patients with SCLC will have limited-stage (LS) disease, which is potentially curable with the combination of chemotherapy and radiation therapy. The standard therapy for LS-SCLC is concurrent chemoradiotherapy, and the 5-year survival rate observed in clinical trials is approximately 25%. The standard chemotherapy remains cisplatin and etoposide, but carboplatin is frequently used in patients who cannot tolerate or have a contraindication to cisplatin. Substantial improvements in survival have been made through improvements in radiation therapy. Concurrent chemoradiotherapy is the preferred therapy for patients who are appropriate candidates. The optimal timing of concurrent chemoradiotherapy is during the first or second cycle, based on data from meta-analyses. The optimal radiation schedule and dose remain topics of debate, but 1.5 Gy twice daily to a total of 45 Gy and 1.8-2.0 Gy daily to a total dose of 60-70 Gy are commonly used treatments. For patients who obtain a near complete or complete response, prophylactic cranial radiation reduces the incidence of brain metastases and improves overall survival. The ongoing Radiation Therapy Oncology Group and Cancer and Leukemia Group B and the European and Canadian phase III trials will investigate different radiation treatment paradigms for patients with LS-SCLC, and completion of these trials is critical.
Conflict of interest statement
The article discusses the use of irinotecan, cisplatin, and etoposide for the treatment of limited-stage small cell lung cancer.
The content of this article has been reviewed by independent peer reviewers to ensure that it is balanced, objective, and free from commercial bias. No financial relationships relevant to the content of this article have been disclosed by the authors or independent peer reviewers.
Figures
References
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2009. CA Cancer J Clin. 2009;59:225–249. - PubMed
-
- Govindan R, Page N, Morgensztern D, et al. Changing epidemiology of small-cell lung cancer in the United States over the last 30 years: Analysis of the Surveillance, Epidemiologic, and End Results database. J Clin Oncol. 2006;24:4539–4544. - PubMed
-
- Gaspar LE, Gay EG, Crawford J, et al. Limited-stage small-cell lung cancer (stages I-III): Observations from the National Cancer Data Base. Clin Lung Cancer. 2005;6:355–360. - PubMed
-
- Turrisi AT, 3rd, Kim K, Blum R, et al. Twice-daily compared with once-daily thoracic radiotherapy in limited small-cell lung cancer treated concurrently with cisplatin and etoposide. N Engl J Med. 1999;340:265–271. - PubMed
-
- Zelen M. Keynote address on biostatistics and data retrieval. Cancer Chemother Rep 3. 1973;4:31–42. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
