

Inhibition of inducible nitric oxide synthase prevents mitochondrial damage and improves survival of steatotic partial liver grafts
- PMID: 20145519
- PMCID: PMC2825166
- DOI: 10.1097/TP.0b013e3181c99185
Inhibition of inducible nitric oxide synthase prevents mitochondrial damage and improves survival of steatotic partial liver grafts
Abstract
Background: Steatotic liver grafts are excluded for partial liver transplantation because of increased risk of primary nonfunction. Mechanisms underlying the failure of fatty partial liver grafts (FPG) remain unknown. This study investigated whether inducible nitric oxide synthase (iNOS) plays a role in failure of FPG.
Methods: Fatty livers were induced by feeding rats a high-fat high-fructose diet for 2 weeks. Hepatic triglyceride was approximately 9-fold higher in rats fed the high-fat high-fructose diet than those fed a low-fat low-fructose diet. Lean and fatty liver explants were reduced in size ex vivo to approximately one third, stored in the University of Wisconsin cold storage solution for 2 hr, and implanted.
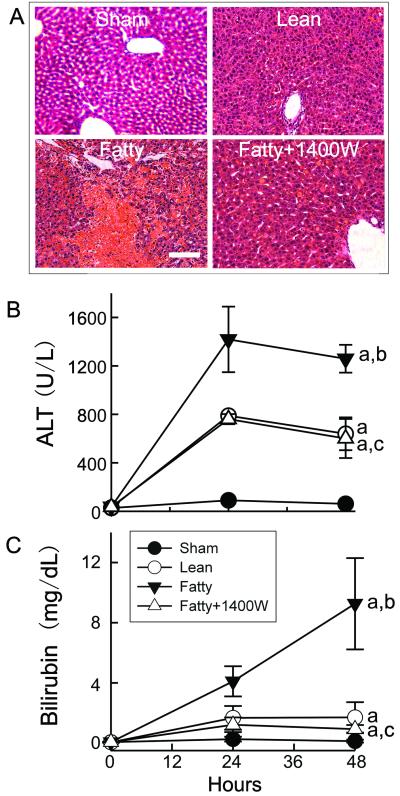
Results: Posttransplantational hepatic iNOS expression and reactive nitrogen species (RNS) formation (nitrite and nitrate levels and 3-nitrotyrosine adducts) increased more profoundly in FPG than in lean partial grafts (LPG). Serum alanine aminotransferase and bilirubin were 2- and 5.5-fold higher after transplantation of FPG than LPG. 5-Bromo-2'-deoxyuridine incorporation was 25% in LPG but only 5% in FPG, and graft weight increased by 64% in LPG while remaining unchanged in FPG. All rats that received FPG died, whereas all those receiving LPG survived. N-(1-naphtyl)ethylendiamine dihydrochloride (5 microM), a specific iNOS inhibitor, largely blunted the production of RNS, prevented the increase of alanine aminotransferase and bilirubin, restored liver regeneration, and improved survival of FPG. Mitochondrial cytochrome c oxidase-IV, ATP synthase-beta, and NADH dehydrogenase-3 decreased markedly in FPG, and these effects were blocked by N-(1-naphtyl)ethylendiamine dihydrochloride.
Conclusion: Thus, hepatic steatosis causes failure of partial liver grafts, most likely by increasing RNS that leads to mitochondrial damage and dysfunction.
Figures





References
-
- Hashimoto K, Miller C. The use of marginal grafts in liver transplantation. J Hepatobiliary Pancreat Surg. 2008;15:92–101. - PubMed
-
- Strong RW. Living-donor liver transplantation: an overview. J Hepatobiliary Pancreat Surg. 2006;13:370–377. - PubMed
-
- Sugawara Y, Makuuchi M, Takayama T, et al. Small-for-size grafts in living-related liver transplantation. J Am Coll Surg. 2001;192:510–513. - PubMed
-
- Kiuchi T, Kasahara M, Uryuhara K, et al. Impact of graft size mismatching on graft prognosis in liver transplantation from living donors. Transplantation. 1999;67:321–327. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
