

Absolute arterial cerebral blood volume quantification using inflow vascular-space-occupancy with dynamic subtraction magnetic resonance imaging
- PMID: 20145656
- PMCID: PMC2949227
- DOI: 10.1038/jcbfm.2010.16
Absolute arterial cerebral blood volume quantification using inflow vascular-space-occupancy with dynamic subtraction magnetic resonance imaging
Abstract
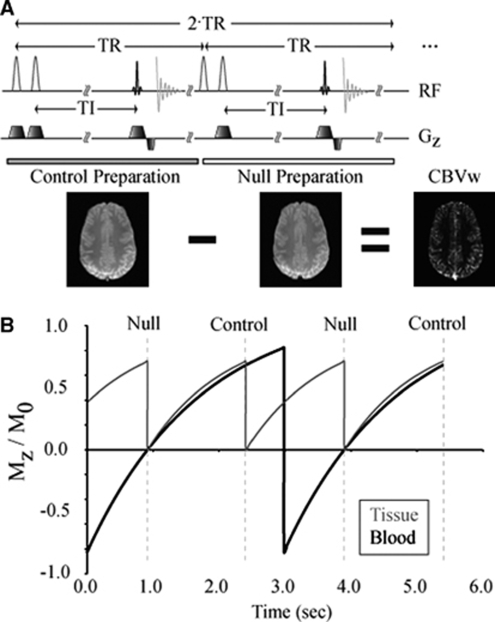
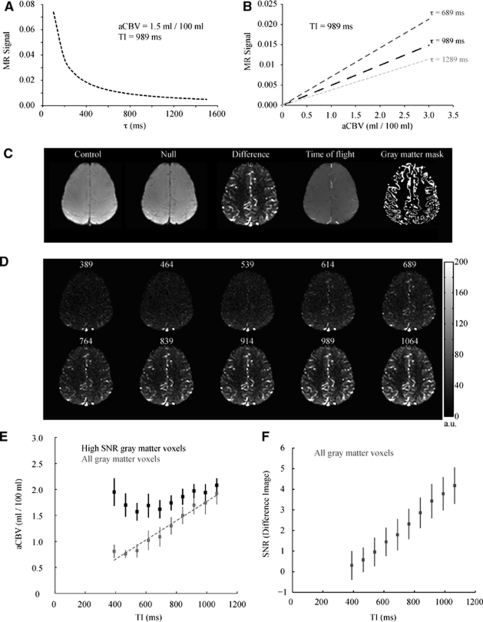
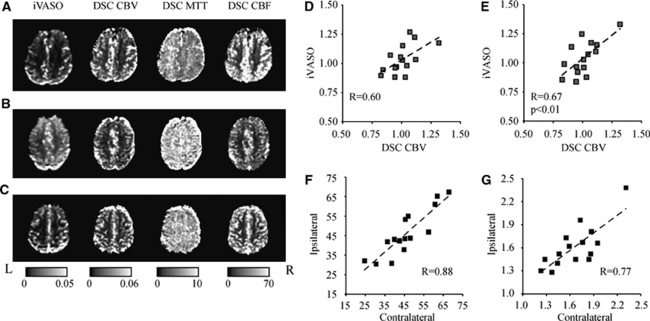
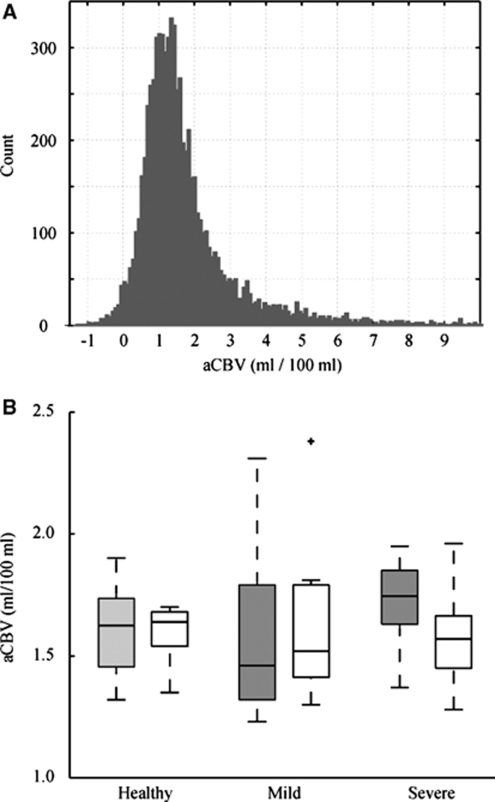
In patients with steno-occlusive disease of the internal carotid artery (ICA), cerebral blood flow may be maintained by autoregulatory increases in arterial cerebral blood volume (aCBV). Therefore, characterizing aCBV may be useful for understanding hemodynamic compensation strategies. A new 'inflow vascular-space-occupancy with dynamic subtraction (iVASO-DS)' MRI approach is presented where aCBV (mL blood/100 mL parenchyma) is quantified without contrast agents using the difference between images with and without inflowing blood water signal. The iVASO-DS contrast mechanism is investigated (3.0 T, spatial resolution=2.4 x 2.4 x 5 mm(3)) in healthy volunteers (n=8; age=29+/-5 years), and patients with mild (n=7; age=72+/-8 years) and severe (n=10; age=73+/-8 years) ICA stenoses. aCBV was quantified in right and left hemispheres in controls, and, alongside industry standard dynamic susceptibility contrast (DSC), contralateral (cont), and ipsilateral (ips) to maximum stenosis in patients. iVASO contrast significantly correlated (R=0.67, P<0.01) with DSC-CBV after accounting for transit time discrepancies. Gray matter aCBV (mL/100 mL) was 1.60+/-0.10 (right) versus 1.61+/-0.20 (left) in controls, 1.59+/-0.38 (cont) and 1.65+/-0.37 (ips) in mild stenosis patients, and 1.72+/-0.18 (cont) and 1.58+/-0.20 (ips) in severe stenosis patients. aCBV was asymmetric (P<0.01) in 41% of patients whereas no asymmetry was found in any control. The potential of iVASO-DS for autoregulation studies is discussed in the context of existing hemodynamic literature.
Figures
Similar articles
-
Inflow-vascular space occupancy (iVASO) reproducibility in the hippocampus and cortex at different blood water nulling times.Magn Reson Med. 2016 Jun;75(6):2379-87. doi: 10.1002/mrm.25836. Epub 2015 Jul 20. Magn Reson Med. 2016. PMID: 26192478 Free PMC article.
-
Hippocampal arterial cerebral blood volume in early psychosis.Psychiatry Res Neuroimaging. 2016 Oct 30;256:21-25. doi: 10.1016/j.pscychresns.2016.09.002. Epub 2016 Sep 9. Psychiatry Res Neuroimaging. 2016. PMID: 27644028 Free PMC article.
-
Noninvasive imaging of cerebral blood volume in piglets with vascular occupancy MR imaging and inflow vascular space occupancy with dynamic subtraction.Magn Reson Imaging. 2018 Jul;50:54-60. doi: 10.1016/j.mri.2018.03.009. Epub 2018 Mar 11. Magn Reson Imaging. 2018. PMID: 29540331
-
Cerebral hemodynamics in asymptomatic patients with internal carotid artery occlusion: a dynamic susceptibility contrast MR and transcranial Doppler study.AJNR Am J Neuroradiol. 2001 Jun-Jul;22(6):1062-7. AJNR Am J Neuroradiol. 2001. PMID: 11415898 Free PMC article.
-
Vascular space occupancy (VASO) cerebral blood volume-weighted MRI identifies hemodynamic impairment in patients with carotid artery disease.J Magn Reson Imaging. 2009 Mar;29(3):718-24. doi: 10.1002/jmri.21667. J Magn Reson Imaging. 2009. PMID: 19243067 Free PMC article.
Cited by
-
Noise concerns and post-processing procedures in cerebral blood flow (CBF) and cerebral blood volume (CBV) functional magnetic resonance imaging.Neuroimage. 2017 Jul 1;154:43-58. doi: 10.1016/j.neuroimage.2016.09.007. Epub 2016 Sep 11. Neuroimage. 2017. PMID: 27622397 Free PMC article. Review.
-
Increased cerebral blood volume in small arterial vessels is a correlate of amyloid-β-related cognitive decline.Neurobiol Aging. 2019 Apr;76:181-193. doi: 10.1016/j.neurobiolaging.2019.01.001. Epub 2019 Jan 10. Neurobiol Aging. 2019. PMID: 30738323 Free PMC article.
-
Quantitative transport mapping (QTM) of the kidney with an approximate microvascular network.Magn Reson Med. 2021 Apr;85(4):2247-2262. doi: 10.1002/mrm.28584. Epub 2020 Nov 18. Magn Reson Med. 2021. PMID: 33210310 Free PMC article.
-
Abnormal arteriolar blood volume measured by 3D inflow-based vascular-space-occupancy (iVASO) MRI and resting-state BOLD fluctuations at 7 T in individuals with recent-onset schizophrenia.Psychoradiology. 2025 Feb 7;5:kkaf001. doi: 10.1093/psyrad/kkaf001. eCollection 2025. Psychoradiology. 2025. PMID: 40182309 Free PMC article.
-
Determination of spin compartment in arterial spin labeling MRI.Magn Reson Med. 2011 Jan;65(1):120-7. doi: 10.1002/mrm.22601. Magn Reson Med. 2011. PMID: 20740655 Free PMC article.
References
-
- An H, Lin W. Cerebral venous and arterial blood volumes can be estimated separately in humans using magnetic resonance imaging. Magn Reson Med. 2002;48:583–588. - PubMed
-
- Boysen G. Cerebral hemodynamics in carotid surgery. Acta Neurol Scand Suppl. 1973;52:3–86. - PubMed
-
- Derdeyn CP, Videen TO, Yundt KD, Fritsch SM, Carpenter DA, Grubb RL, Powers WJ. Variability of cerebral blood volume and oxygen extraction: stages of cerebral haemodynamic impairment revisited. Brain. 2002;125:595–607. - PubMed
-
- Donahue MJ, Blicher JU, Ostergaard L, Feinberg DA, Macintosh BJ, Miller KL, Gunther M, Jezzard P. Cerebral blood flow, blood volume, and oxygen metabolism dynamics in human visual and motor cortex asmeasured by whole-brain multi-modal magnetic resonance imaging. J Cereb Blood Flow Metab. 2009a;29:1856–1866. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
