

Management of fall-related injuries in the elderly: a retrospective chart review of patients presenting to the emergency department of a community-based teaching hospital
- PMID: 20145749
- PMCID: PMC2788319
- DOI: 10.3138/physio.61.1.26
Management of fall-related injuries in the elderly: a retrospective chart review of patients presenting to the emergency department of a community-based teaching hospital
Abstract
Purpose: To identify current practice for elderly individuals who have sustained a fall-related injury and subsequently presented to the emergency department (ED) of a community-based hospital in Toronto, Ontario.
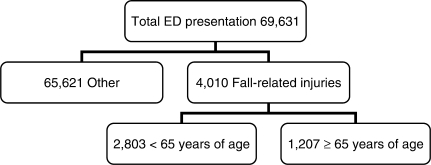
Methods: A retrospective longitudinal chart review was conducted for 300 persons, 65 years of age and older, who presented to the ED of a community-based teaching hospital with a fall from June 2004 through May 2005. Data were collected using a tool created by the investigators (based on information gathered through a literature review) to capture information related to risk factors for falling.
Results: Our study sample was demographically similar to elderly individuals in other fall-related studies. Most patients discharged directly from the ED did not receive multidisciplinary care. In the ED, all patients saw a nurse or physician, while only 1.3% (n = 4) saw a physical therapist, 3.0% (n = 9) saw an occupational therapist, and 5.3% (n = 16) saw a social worker. At discharge, 62% (n = 152) had no documented referral for follow-up care. Abilities related to falls in elderly individuals were not consistently assessed in the ED. Frequency of assessment for these abilities was as follows: (1) gait, 10.2%; (2) balance, 4.1%; (3) lower-extremity range of motion, 4.9%; (4) lower-extremity strength, 2.0%; (5) cognition, 26.1%; (6) vision, 2.0%; (7) ability to perform activities of daily living, 7.3%. In the 6 months following the index fall, 8.3% of patients returned to the ED of the same hospital because of a subsequent fall.
Conclusions: In the ED, fall-related risk factors were not consistently assessed or documented, and few patients received multidisciplinary management. Since elderly individuals who fall commonly present to the ED, the implementation of evidence-based strategies aimed at preventing repeat falls should be considered.
Objectif : Définir les modalités des soins fournis aux personnes âgées qui se sont présentées au service des urgences d'un hôpital communautaire de Toronto, en Ontario, après s'être blessées en tombant.
Méthode : On a procédé à l'analyse rétrospective longitudinale des dossiers de 300 personnes de 65 ans et plus qui s'étaient présentées, de juin 2004 à mai 2005, au service des urgences d'un hôpital communautaire universitaire après avoir fait une chute. La collecte des données s'est effectuée au moyen d'un outil mis au point par les enquêteurs (selon ce qu'a révélé une analyse documentaire), en vue de faire ressortir les facteurs de risque de chute.
Résultats : L'échantillon étudié s'apparentait, sur le plan démographique, à la population des personnes âgées prise en compte dans d'autres études sur le sujet. La plupart des patients qui ont été congédié directement du service des urgences n'ont pas eu accès à des soins multidisciplinaires. Tous ont pu consulter un médecin ou un membre du personnel infirmier, mais à peine 1,3 % (n = 4) ont vu un physiothérapeute, 3,0 % (n = 9), un ergothérapeute et 5,3 % (n = 16), un travailleur social. Au congé, 62 % des patients (n = 152) n'avaient reçu aucune demande de consultation écrite aux fins de suivi. Au service des urgences, les aptitudes jouant un rôle dans les chutes, plutôt que de faire l'objet d'une évaluation systématique, ont été mesurées à des fréquences diverses : (1) démarche = 10,2 %; (2) équilibre = 4,1 %; (3) amplitude de mouvement des membres inférieurs = 4,9 %; (4) force des membres inférieurs = 2,0 %; (5) cognition = 26,1 %; (6) vision = 2,0 %; (7) capacité de d'exécuter les activités de la vie quotidienne = 7,3 %. Au cours des 6 mois qui ont suivi la chute de référence, une autre chute a obligé 8,3 % des patients à se rendre de nouveau au service des urgences du même hôpital.
Conclusions : Les facteurs de risque de chute n'ont pas été systématiquement évalués et/ou documentés, et peu de patients ont bénéficié d'une prise en charge multidisciplinaire après s'être présentés au service des urgences. Comme il est fréquent que des personnes âgées se rendent au service des urgences après une chute, la mise en place de stratégies fondées sur des données probantes et destinées à prévenir les chutes à répétition devrait être envisagée.
Keywords: emergency department management; fall prevention; fall risk; fall-related injuries; falls in the elderly.
Figures
Similar articles
-
Evaluation of RESPOND, a patient-centred program to prevent falls in older people presenting to the emergency department with a fall: A randomised controlled trial.PLoS Med. 2019 May 24;16(5):e1002807. doi: 10.1371/journal.pmed.1002807. eCollection 2019 May. PLoS Med. 2019. PMID: 31125354 Free PMC article. Clinical Trial.
-
Older adult falls prevention behaviors 60 days post-discharge from an urban emergency department after treatment for a fall.Inj Epidemiol. 2017 Dec;4(1):18. doi: 10.1186/s40621-017-0114-y. Epub 2017 Jun 19. Inj Epidemiol. 2017. PMID: 28626848 Free PMC article.
-
Randomized Controlled Trial of Screening, Risk Modification, and Physical Therapy to Prevent Falls Among the Elderly Recently Discharged From the Emergency Department to the Community: The Steps to Avoid Falls in the Elderly Study.Arch Phys Med Rehabil. 2017 Jun;98(6):1086-1096. doi: 10.1016/j.apmr.2017.01.014. Epub 2017 Feb 12. Arch Phys Med Rehabil. 2017. PMID: 28202383 Clinical Trial.
-
Multifactorial falls prevention programmes for older adults presenting to the emergency department with a fall: systematic review and meta-analysis.Inj Prev. 2019 Dec;25(6):557-564. doi: 10.1136/injuryprev-2019-043214. Epub 2019 Jul 9. Inj Prev. 2019. PMID: 31289112
-
Journey to a safe environment: fall prevention in an emergency department at a level I trauma center.J Emerg Nurs. 2013 Jul;39(4):346-52. doi: 10.1016/j.jen.2012.11.003. Epub 2013 Feb 4. J Emerg Nurs. 2013. PMID: 23380299 Review.
Cited by
-
Investigating the Association between Outdoor Environment and Outdoor Activities for Seniors Living in Old Residential Communities.Int J Environ Res Public Health. 2021 Jul 14;18(14):7500. doi: 10.3390/ijerph18147500. Int J Environ Res Public Health. 2021. PMID: 34299950 Free PMC article.
-
Return to the ED and hospitalisation following minor injuries among older persons treated in the emergency department: predictors among independent seniors within 6 months.Age Ageing. 2015 Jul;44(4):624-9. doi: 10.1093/ageing/afv054. Epub 2015 May 5. Age Ageing. 2015. PMID: 25944869 Free PMC article.
-
Timed Up and Go predicts functional decline in older patients presenting to the emergency department following minor trauma†.Age Ageing. 2017 Mar 1;46(2):214-218. doi: 10.1093/ageing/afw184. Age Ageing. 2017. PMID: 28399218 Free PMC article.
-
Clinician's Commentary on Arnold and Gyurcsik(1.).Physiother Can. 2012 Summer;64(3):315-6. doi: 10.3138/ptc.2011-12-CC. Physiother Can. 2012. PMID: 23729968 Free PMC article. No abstract available.
-
Evolution of a Level I Trauma System: changes in injury mechanism and its impact in the delivery of care.Int J Burns Trauma. 2011;1(1):56-61. Epub 2011 Sep 3. Int J Burns Trauma. 2011. PMID: 22928159 Free PMC article.
References
-
- Public Health Agency of Canada. Report on seniors' falls in Canada [homepage on the Internet] Ottawa: The Agency; 2005. [updated 2005 Nov 4; cited 2005 Nov 23]. Available from: http://www.phac-aspc.gc.ca/seniors-aines/pubs/seniors_falls/index.htm.
-
- Health Canada. Canada's ageing population [homepage on the Internet] Ottawa: Health Canada; 2002. [cited 2005 Nov 23]. Available from: http://www.phac-aspc.gc.ca/seniors-aines/pubs/fed_paper/pdfs/fedpager_e.pdf.
-
- Canadian Orthopaedic Association. Canada in motion: mobilizing access to orthopaedic care [homepage on the Internet] 2005. [updated 2008 Feb 11; cited 2008 Oct 23]. Available from: http://www.coa-aco.org/library/health_policy/canada_in_motion.html.
-
- American Geriatrics Society, British Geriatrics Society, American Academy of Orthopaedic Surgeons Panel on Falls Prevention. Guideline for the prevention of falls in older persons. J Am Geriatr Soc. 2001;49:664–72. - PubMed
-
- Manitoba Health. Preventing falls and fall-related injuries in Manitoba: a review of best practices. Impact. 2005:18–30.
LinkOut - more resources
Full Text Sources