

Carbonized blood deposited on fibres during 810, 940 and 1,470 nm endovenous laser ablation: thickness and absorption by optical coherence tomography
- PMID: 20145968
- PMCID: PMC2834766
- DOI: 10.1007/s10103-009-0749-1
Carbonized blood deposited on fibres during 810, 940 and 1,470 nm endovenous laser ablation: thickness and absorption by optical coherence tomography
Abstract
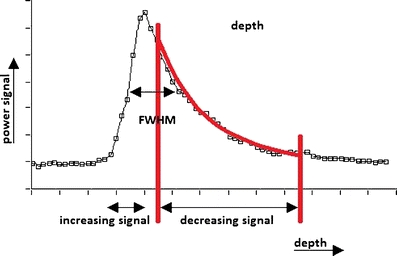
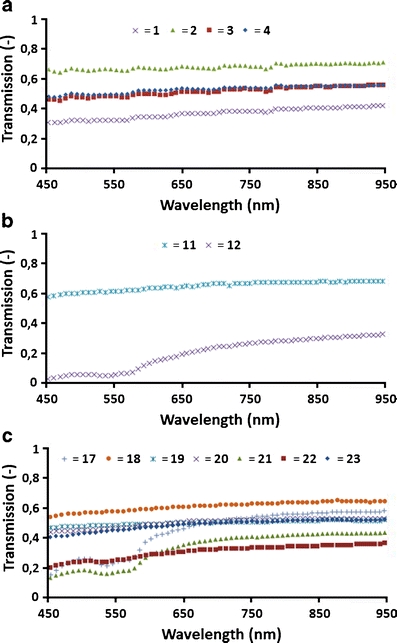
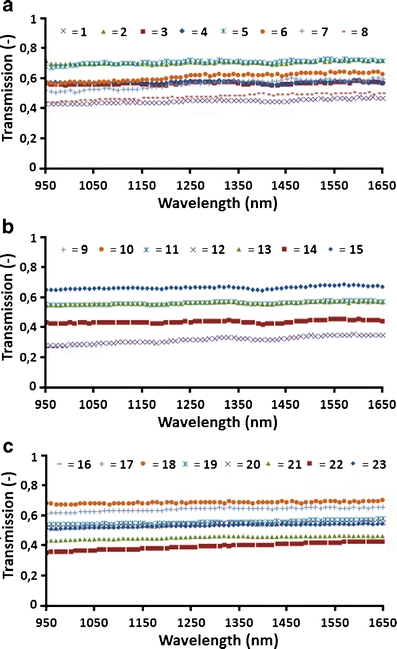
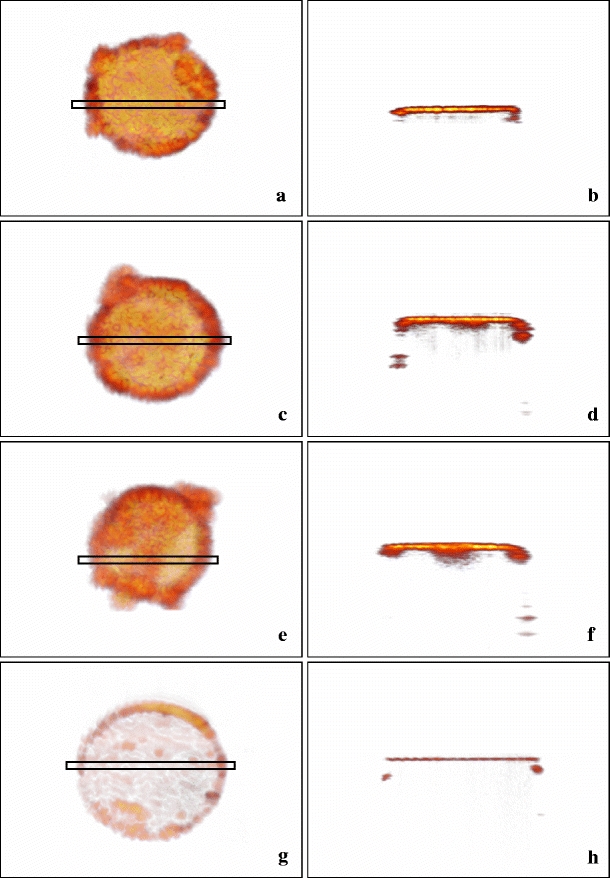
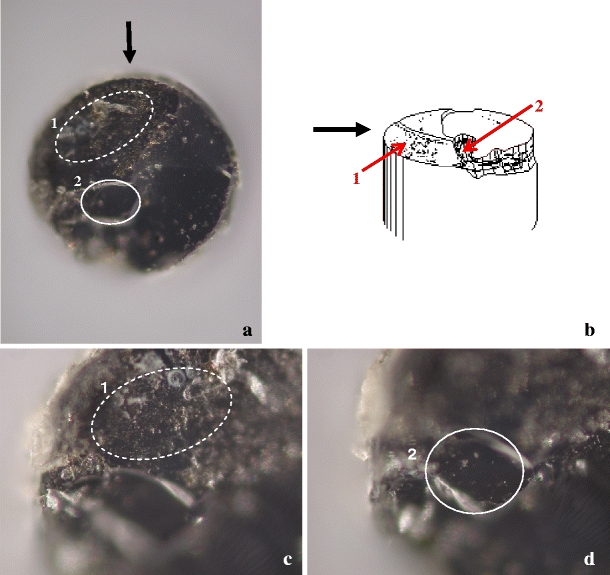
Endovenous laser ablation (EVLA) is commonly used to treat saphenous varicosities. Very high temperatures at the laser fibre tip have been reported during EVLA. We hypothesized that the laser irradiation deposits a layer of strongly absorbing carbonized blood of very high temperature on the fibre tip. We sought to prove the existence of these layers and study their properties by optical transmission, optical coherence tomography (OCT) and microscopy. We analysed 23 EVLA fibres, 8 used at 810 nm, 7 at 940 nm and 8 at 1,470 nm. We measured the transmission of these fibres in two wavelength bands (450-950 nm; 950-1,650 nm). We used 1,310 nm OCT to assess the thickness of the layers and the attenuation as a function of depth to determine the absorption coefficient. Microscopy was used to view the tip surface. All fibres showed a slightly increasing transmission with wavelength in the 450-950 nm band, and a virtually wavelength-independent transmission in the 950-1,650 nm band. OCT scans showed a thin layer deposited on all 13 fibres investigated, 6 used at 810 nm, 4 at 940 nm and 3 at 1,470 nm, some with inhomogeneities over the tip area. The average absorption coefficient of the 13 layers was 72 +/- 16 mm(-1). The average layer thickness estimated from the transmission and absorption measurements was 8.0 +/- 2.7 microm. From the OCT data, the average maximal thickness was 26 +/- 6 microm. Microscopy of three fibre tips, one for each EVLA wavelength, showed rough, cracked and sometimes seriously damaged tip surfaces. There was no clear correlation between the properties of the layers and the EVLA parameters such as wavelength, except for a positive correlation between layer thickness and total delivered energy. In conclusion, we found strong evidence that all EVLA procedures in blood filled veins deposit a heavily absorbing hot layer of carbonized blood on the fibre tip, with concomitant tip damage. This major EVLA mechanism is unlikely to have much wavelength dependence at similar delivered energies per centimetre of vein. Optical-thermal interaction between the vein wall and the transmitted laser light depends on wavelength.
Figures
References
-
- Proebstle TM, Lehr HA, Kargl A, Espinola-Klein C, Rother W, Bethge S, Knop J. Endovenous treatment of the greater saphenous vein with a 940 nm diode laser: thrombotic occlusion after endoluminal thermal damage by laser-generated steam bubbles. J Vasc Surg. 2002;35:729–736. doi: 10.1067/mva.2002.121132. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
