

Lessons learned from a randomized trial of airway secretion clearance techniques in cystic fibrosis
- PMID: 20146387
- PMCID: PMC4163837
- DOI: 10.1002/ppul.21179
Lessons learned from a randomized trial of airway secretion clearance techniques in cystic fibrosis
Abstract
Rationale: Airway secretion clearance therapies are a cornerstone of cystic fibrosis care, however longitudinal comparative studies are rare. Our objectives were to compare three therapies [postural drainage and percussion: (postural drainage), flutter device (FD), and high frequency chest wall oscillation: (vest)], by studying (1) change in pulmonary function; (2) time to need for intravenous (IV) antibiotics, (3) use of pulmonary therapies, (4) adherence to treatment, (5) treatment satisfaction, and (6) quality of life.
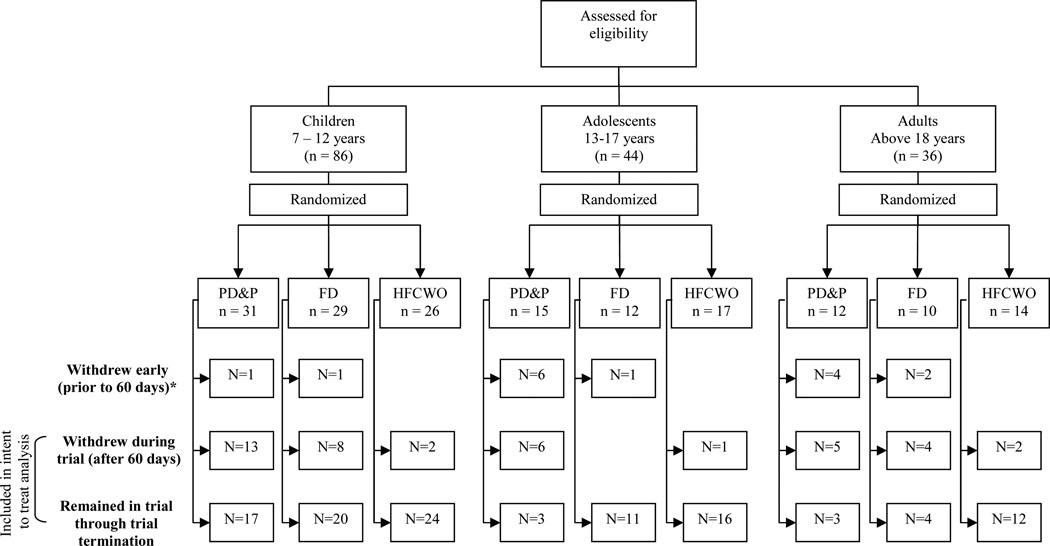
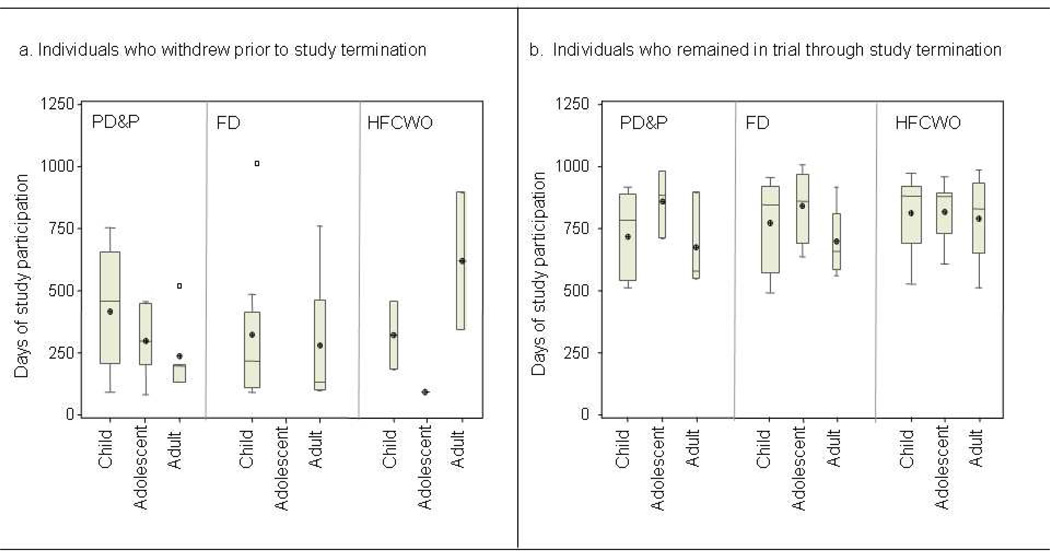
Methods: Participants were randomly assigned to one of three therapies twice daily. Clinical outcomes were assessed quarterly over 3 years.
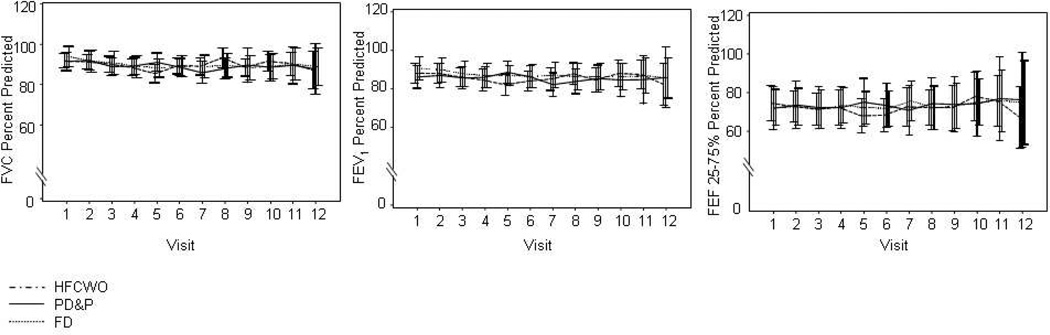
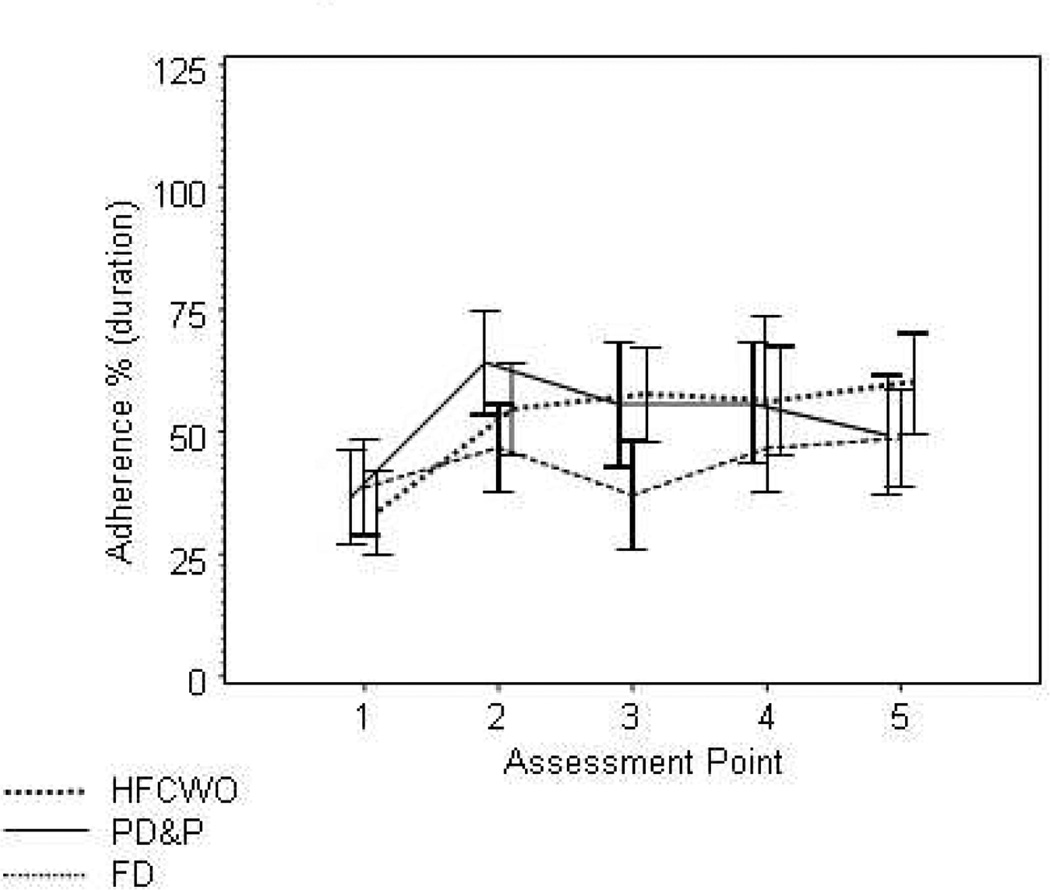
Results: Enrollment goals were not met, and withdrawal rates were high, especially in postural drainage (51%) and FD (26%), compared to vest (9%), resulting in early termination. FEV(1) decline, time to need IV antibiotics, and other pulmonary therapies were not different. The annual FEF(25-75%) predicted rate of decline was greater in those using vest (P = 0.02). Adherence was not significantly different (P = 0.09). Overall treatment satisfaction was higher in vest and FD than in postural drainage (P < 0.05). Health-related quality of life was not different. The rate of FEV(1) decline was 1.23% predicted/year.
Conclusions: The study was ended early due to dropout and smaller than expected decline in FEV(1). Patients were more satisfied with vest and FD. The longitudinal decline in FEF(25-75%) was faster in vest; we found no other difference in lung function decline, taken together this warrants further study. The slow decline in FEV(1) illustrates the difficulty with FEV(1) decline as a clinical trial outcome.
Figures
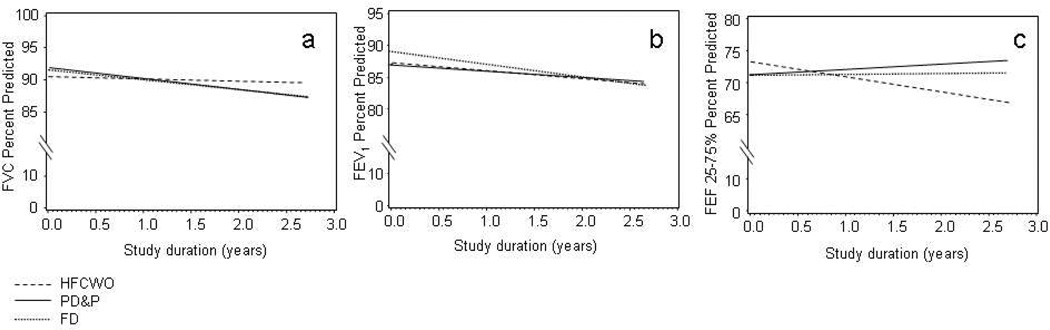
Panel a: FVC % Predicted
PD&P: y=85.1 (± 2.7 SEM) − 1.5 (± 0.94) *years in study + 0.13*BMI%
FD: y=85.6 (± 2.8 SEM) − 1.7 (± 0.89) *years in study + 0.13*BMI%
HFCWO: y=84.2 (± 2.7 SEM) − 0.32 (± 0.77 SEM) *years in study + 0.13*BMI%
p=NS, comparison of all slopes
Panel b: FEV1 % Predicted
PD&P: y=80.3 (± 3.6 SEM) − 1.0 (± 0.96) *years in study + 0.14*BMI%
FD:: y=82.3 (± 3.7 SEM) – 1.9 (± 0.91) *years in study + 0.14*BMI%
HFCWO: y=80.4 (± 3.5 SEM) – 1.20 (± 0.78 SEM)*years in study + 0.14*BMI%
p=NS, comparison of all slopes
Panel c: FEF 25–75% % Predicted
PD&P: y=71.2 (± 4.7 SEM) + 0.85 (± 0.99) *years in study
FD: y=71.1 (± 4.7 SEM) – 0.16 (± 0.90) *years in study
HFCWO: y=73.1 (± 4.3 SEM) – 2.32 (± 0.76 SEM) *years in study
p=0.01 PD&P vs HFCWO, p=0.035 FD vs. HFCWO

References
-
- Davis PB. Cystic fibrosis since 1938. Am J Respir Crit Care Med. 2006;173(5):475–482. - PubMed
-
- Tarran R, Button B, Picher M, Paradiso AM, Ribeiro CM, Lazarowski ER, Zhang L, Collins PL, Pickles RJ, Fredberg JJ, Boucher RC. Normal and cystic fibrosis airway surface liquid homeostasis. The effects of phasic shear stress and viral infections. J Biol Chem. 2005;280(42):35751–35759. - PMC - PubMed
-
- Gibson RL, Burns JL, Ramsey BW. Pathophysiology and management of pulmonary infections in cystic fibrosis. Am J Respir Crit Care Med. 2003;168(8):918–951. - PubMed
-
- van der SC, Prasad A, Main E. Chest physiotherapy compared to no chest physiotherapy for cystic fibrosis. Cochrane Database Syst Rev. 2000;2:CD001401. - PubMed
-
- McIlwaine PM, Wong LT, Peacock D, Davidson AG. Long-term comparative trial of conventional postural drainage and percussion versus positive expiratory pressure physiotherapy in the treatment of cystic fibrosis. J Pediatr. 1997;131(4):570–574. [see comments]. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
