

Risk scoring systems for adults admitted to the emergency department: a systematic review
- PMID: 20146829
- PMCID: PMC2835641
- DOI: 10.1186/1757-7241-18-8
Risk scoring systems for adults admitted to the emergency department: a systematic review
Abstract
Background: Patients referred to a medical admission unit (MAU) represent a broad spectrum of disease severity. In the interest of allocating resources to those who might potentially benefit most from clinical interventions, several scoring systems have been proposed as a triaging tool.Even though most scoring systems are not meant to be used on an individual level, they can support the more inexperienced doctors and nurses in assessing the risk of deterioration of their patients.We therefore performed a systematic review on the level of evidence of literature on scoring systems developed or validated in the MAU. We hypothesized that existing scoring systems would have a low level of evidence and only few systems would have been externally validated.
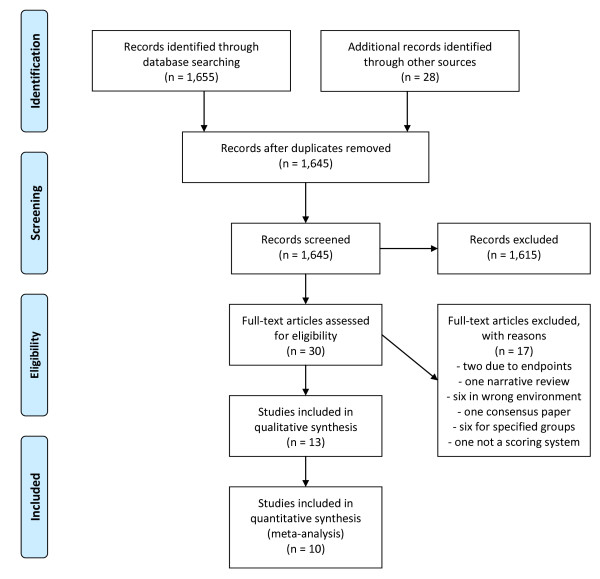
Methods: We conducted a systematic search using Medline, EMBASE and the Cochrane Library, according to the PRISMA guidelines, on scoring systems developed to assess medical patients at admission.The primary endpoints were in-hospital mortality or transfer to the intensive care unit. Studies derived for only a single or few diagnoses were excluded.The ability to identify patients at risk (discriminatory power) and agreement between observed and predicted outcome (calibration) along with the method of derivation and validation (application on a new cohort) were extracted.
Results: We identified 1,655 articles. Thirty were selected for further review and 10 were included in this review.Eight systems used vital signs as variables and two relied mostly on blood tests.Nine systems were derived using regression analysis and eight included patients admitted to a MAU. Six systems used in-hospital mortality as their primary endpoint.Discriminatory power was specified for eight of the scoring systems and was acceptable or better in five of these. The calibration was only specified for four scoring systems. In none of the studies impact analysis or inter-observer reliability were analyzed.None of the systems reached the highest level of evidence.
Conclusions: None of the 10 scoring systems presented in this article are perfect and all have their weaknesses. More research is needed before the use of scoring systems can be fully implemented to the risk assessment of acutely admitted medical patients.
Figures
References
-
- Vincent JL, Moreno R, Takala J, Willatts S, de MA, Bruining H. et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996;18:707–710. doi: 10.1007/BF01709751. - DOI - PubMed
-
- PRISMA Statement. 2010. http://www.prisma-statement.org/ Ref Type: Internet Communication.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
