

CO and NO pulmonary diffusing capacity during pregnancy: Safety and diagnostic potential
- PMID: 20149901
- PMCID: PMC3725751
- DOI: 10.1016/j.resp.2010.02.001
CO and NO pulmonary diffusing capacity during pregnancy: Safety and diagnostic potential
Abstract
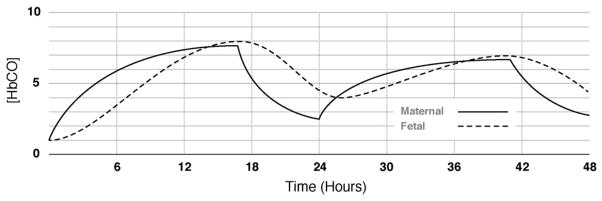
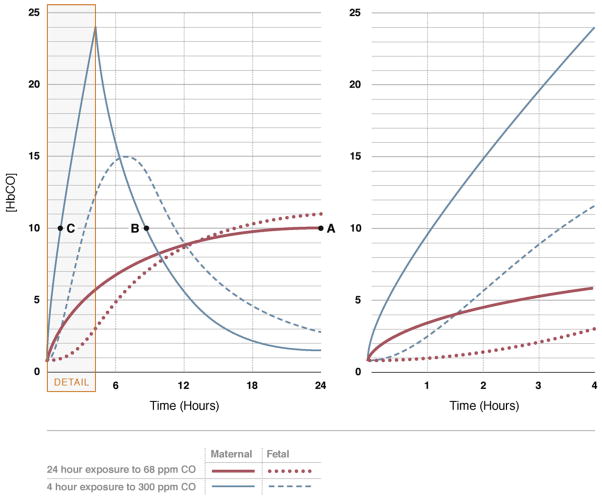
This paper reviews the scientific evidence for the safety of carbon monoxide (CO) and nitric oxide (NO) inhalation to measure pulmonary diffusing capacity (DL(CO) and DL(NO)) in pregnant women and their fetuses. In eight earlier studies, 650 pregnant women had DL(CO) measurements performed at various times during pregnancy, with a minimum of two to four tests per session. Both pregnant subjects that were healthy and those with medical complications were tested. No study reported adverse maternal, fetal, or neonatal outcomes from the CO inhalation in association with measuring DL(CO). Eleven pregnant women, chiefly with pulmonary hypertension, and 1105 pre-term neonates, mostly with respiratory failure, were administered various dosages of NO (5-80ppm for 4 weeks continuously in pregnant women, and 1-20ppm for 15min to 3 weeks for the neonates). NO treatment was found to be an effective therapy for pregnant women with pulmonary hypertension. In neonates with respiratory failure and pulmonary hypertension, NO therapy improved oxygenation and survival and has been associated with only minor, transient adverse effects. In conclusion, maternal carboxyhemoglobin ([Hb(CO)]) levels can safely increase to 5% per testing session when the dose-exposure limit is 0.3% CO inhalation for <or=3min, and for NO, 80ppm for <or=3min. The risk of late fetal or neonatal death from increased Hb(CO) from diffusion testing is considerably less than the risk of death from all causes reported by the Centers for Disease Control, and is therefore considered "minimal risk".
Copyright 2010 Elsevier B.V. All rights reserved.
Conflict of interest statement
No author has any actual or potential conflicts of interest pertaining to this manuscript.
Figures
References
-
- ACSM. ACSM’s Guidelines for Exercise Testing and Prescription. 8. Lippincott Williams & Wilkins; Baltimore: 2009.
-
- Alaily AB, Carrol KB. Pulmonary ventilation in pregnancy. Br J Obstet Gynaecol. 1978;85:518–524. - PubMed
-
- Amitai Y, Zlotogorski Z, Golan-Katzav V, Wexler A, Gross D. Neuropsychological impairment from acute low-level exposure to carbon monoxide. Arch Neurol. 1998;55:845–848. - PubMed
-
- Baldwin GR, Moorthi DS, Whelton JA, MacDonnell KF. New lung functions and pregnancy. Am J Obstet Gynecol. 1977;127:235–239. - PubMed
-
- Barker SJ, Curry J, Redford D, Morgan S. Measurement of carboxyhemoglobin and methemoglobin by pulse oximetry: a human volunteer study. Anesthesiology. 2006;105:892–897. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
