

The timing of cranial radiation in elderly patients with newly diagnosed glioblastoma multiforme
- PMID: 20150386
- PMCID: PMC2940582
- DOI: 10.1093/neuonc/nop004
The timing of cranial radiation in elderly patients with newly diagnosed glioblastoma multiforme
Abstract
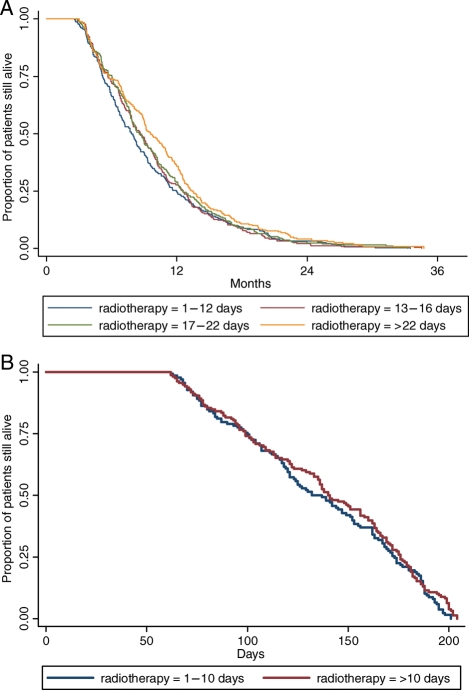
There are few and conflicting studies on the optimal timing of initial cranial radiation in the treatment of glioblastoma multiforme (GBM) but none of them have addressed this issue in the elderly population. We used the linked Surveillance, Epidemiology, and End Results (SEER) Medicare database to investigate whether the time interval from surgery to initiation of radiation is a significant prognostic factor for survival in subjects aged > or =65 years with newly diagnosed GBM. Cox modeling was used to assess the effect of waiting time on overall survival. We identified a total of 1,375 patients, 296 with biopsies and 1,079 with resections. The median time to the initiation of radiotherapy was 15 days post operation (interquartile range 12-21). In the univariate Cox analysis of those who had debulking surgeries, a waiting time of >22 days showed a significant inverse relationship with survival (hazard ratio [HR] = 0.82, 95% CI 0.70-0.97, p = 0.02), but after adjustment for confounders, it was not a statistically significant factor in the final Cox model (HR = 0.99, 95% CI 0.97-1.01, p = 0.14). Therefore, waiting time was not a significant prognostic factor for subjects with biopsies in both the univariate and multivariate analyses. Although effort should be made to initiate radiotherapy as soon as possible after surgical resection/biopsy, a brief delay similar to that experienced by our cohort does not have a significant impact on survival.
Figures
References
-
- Keime-Guibert F, Chinot O, Taillandier L, et al. Radiotherapy for glioblastoma in the elderly. N Engl J Med. 2007;356:1527–1535. - PubMed
-
- Roa W, Brasher PM, Bauman G, et al. Abbreviated course of radiation therapy in older patients with glioblastoma multiforme: a prospective randomized clinical trial. J Clin Oncol. 2004;22:1583–1588. - PubMed
-
- Burnet NG, Jena R, Jefferies SJ, et al. Mathematical modelling of survival of glioblastoma patients suggests a role for radiotherapy dose escalation and predicts poorer outcome after delay to start treatment. Clin Oncol (R Coll Radiol) 2006;18:93–103. - PubMed
-
- Mirimanoff RO, Gorlia T, Mason W, et al. Radiotherapy and temozolomide for newly diagnosed glioblastoma: recursive partitioning analysis of the EORTC 26981/22981-NCIC CE3 Phase III Randomized Trial. J Clin Oncol. 2006;24:2563–2569. - PubMed
-
- Irwin C, Hunn M, Purdie G, et al. Delay in radiotherapy shortens survival in patients with high-grade glioma. J Neurooncol. 2007;85:339–343. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
