

The prevalence and clinical course of HIV-associated pulmonary cryptococcosis in Uganda
- PMID: 20150818
- PMCID: PMC2892206
- DOI: 10.1097/QAI.0b013e3181ce6b19
The prevalence and clinical course of HIV-associated pulmonary cryptococcosis in Uganda
Abstract
Background: The prevalence and clinical course of pulmonary cryptococcosis in Sub-Saharan Africa are not well described.
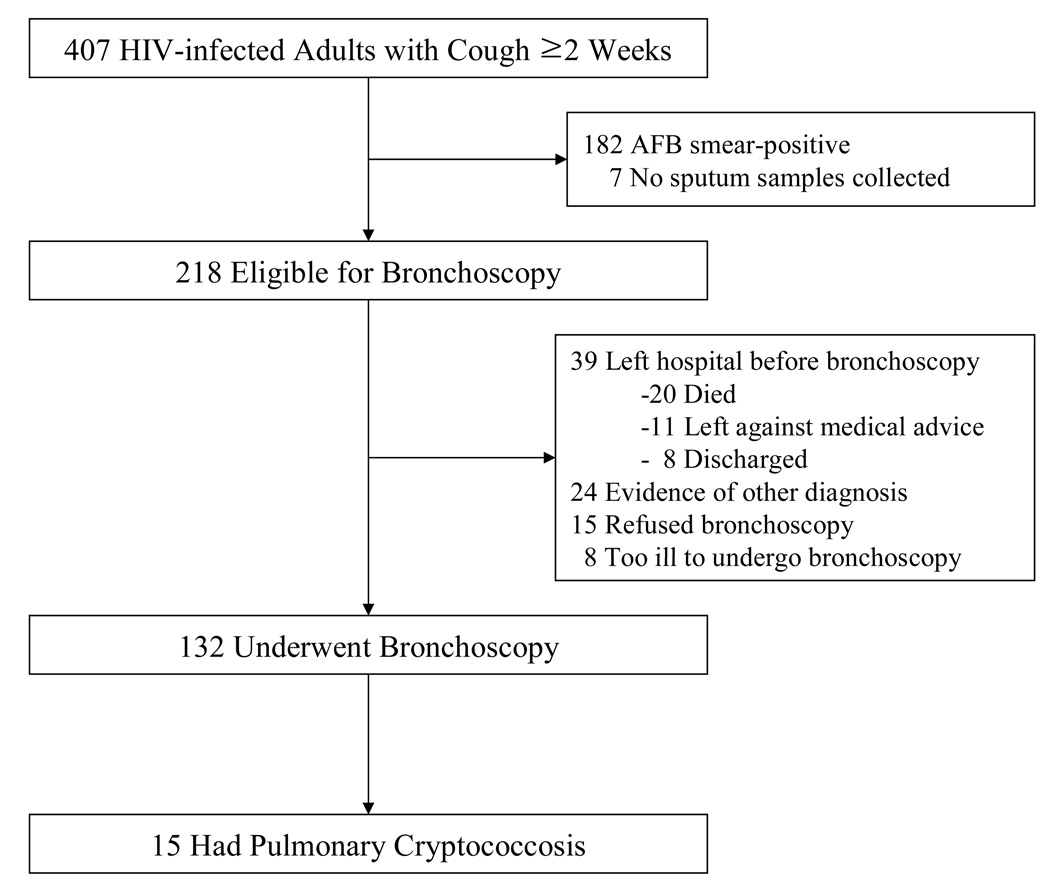
Methods: Consecutive HIV-infected adults hospitalized at Mulago Hospital (Kampala, Uganda) between September 2007 and July 2008 with cough >or=2 weeks were enrolled. Patients with negative sputum smears for acid-fast bacilli were referred for bronchoscopy with bronchoalveolar lavage (BAL). BAL fluid was examined for mycobacteria, Pneumocystis jirovecii, and fungi. Patients were followed 2 and 6 months after hospital discharge.
Results: Of 407 patients enrolled, 132 (32%) underwent bronchoscopy. Of 132 BAL fungal cultures, 15 (11%) grew Cryptococcus neoformans. None of the patients were suspected to have pulmonary cryptococcosis on admission. The median CD4 count among those with pulmonary cryptococcosis was 23 cells per microliter (interquartile range = 7-51). Of 13 patients who completed 6-month follow-up, 4 died and 9 were improved, including 5 who had started antiretroviral therapy but had not received antifungal medication.
Conclusions: Pulmonary cryptococcosis is common in HIV-infected tuberculosis suspects in Uganda. Early initiation of antiretroviral therapy in those with isolated pulmonary infection may improve outcomes, even without antifungal therapy. This finding suggests that some HIV-infected patients with C. neoformans isolated from respiratory samples may have colonization or localized infection.
Figures
Similar articles
-
Prevalence and outcomes of cryptococcal antigenemia in HIV-seropositive patients hospitalized for suspected tuberculosis in Uganda.J Acquir Immune Defic Syndr. 2013 Jun 1;63(2):189-94. doi: 10.1097/QAI.0b013e3182926f95. J Acquir Immune Defic Syndr. 2013. PMID: 23542636 Free PMC article.
-
Clinical significance of normal chest radiographs among HIV-seropositive patients with suspected tuberculosis in Uganda.Respirology. 2011 Jul;16(5):836-41. doi: 10.1111/j.1440-1843.2011.01981.x. Respirology. 2011. PMID: 21518124 Free PMC article.
-
[Cryptococcosis--a common fungal infection in immunosuppressed patient].Pneumologia. 2014 Jul-Sep;63(3):156, 159-63. Pneumologia. 2014. PMID: 25420290 Review. Romanian.
-
Prevalence of cryptococcosis among HIV-infected patients in Yaounde, Cameroon.Afr Health Sci. 2012 Jun;12(2):129-33. doi: 10.4314/ahs.v12i2.8. Afr Health Sci. 2012. PMID: 23056017 Free PMC article.
-
Current approach to the acute management of cryptococcal infections.J Infect. 2000 Jul;41(1):18-22. doi: 10.1053/jinf.2000.0696. J Infect. 2000. PMID: 11041709 Review. No abstract available.
Cited by
-
Cryptococcosis with pulmonary cavitation in an immunocompetent child: a case report and literature review.BMC Infect Dis. 2024 Feb 6;24(1):162. doi: 10.1186/s12879-024-09061-1. BMC Infect Dis. 2024. PMID: 38321369 Free PMC article. Review.
-
New Insights into HIV/AIDS-Associated Cryptococcosis.ISRN AIDS. 2013 Feb 25;2013:471363. doi: 10.1155/2013/471363. ISRN AIDS. 2013. PMID: 24052889 Free PMC article. Review.
-
Evaluation of antibody responses to panels of M. tuberculosis antigens as a screening tool for active tuberculosis in Uganda.PLoS One. 2017 Aug 2;12(8):e0180122. doi: 10.1371/journal.pone.0180122. eCollection 2017. PLoS One. 2017. PMID: 28767658 Free PMC article.
-
CrAg lateral flow assay for cryptococcosis.Expert Opin Med Diagn. 2012 May;6(3):245-51. doi: 10.1517/17530059.2012.681300. Epub 2012 Apr 19. Expert Opin Med Diagn. 2012. PMID: 23480688 Free PMC article.
-
Pulmonary cryptococcosis presenting as acute severe respiratory distress in a newly diagnosed HIV patient in Tanzania: a case report.Clin Case Rep. 2015 Sep;3(9):749-52. doi: 10.1002/ccr3.337. Epub 2015 Aug 11. Clin Case Rep. 2015. PMID: 26401280 Free PMC article.
References
-
- Kobayashi G. Fungi. In: Davis BD, editor. Microbiology. Philadelphia: J.B: Lippincott Company; 1980. p. 751.
-
- Park BJ, Wannemuehler KA, Marston BJ, et al. Estimation of the current global burden of cryptococcal meningitis among persons living with HIV/AIDS. AIDS. 2009;23(4):525–530. - PubMed
-
- Powderly WG, Finkelstein D, Feinberg J, et al. NIAID AIDS Clinical Trials Group. A randomized trial comparing fluconazole with clotrimazole troches for the prevention of fungal infections in patients with advanced human immunodeficiency virus infection. N Engl J Med. 1995;332(11):700–705. - PubMed
-
- French N, Gray K, Watera C, et al. Cryptococcal infection in a cohort of HIV-1-infected Ugandan adults. AIDS. 2002;16:1031–1038. - PubMed
-
- Churchyard GJ, Kleinschmidt I, Corbett EL, et al. Factors associated with an increased case-fatality rate in HIV-infected and non-infected South African gold miners with pulmonary tuberculosis. Int J Tuberc Lung Dis. 2000;4(8):705–712. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
