

Osteochondral defects in the ankle: why painful?
- PMID: 20151110
- PMCID: PMC2855020
- DOI: 10.1007/s00167-010-1064-x
Osteochondral defects in the ankle: why painful?
Abstract
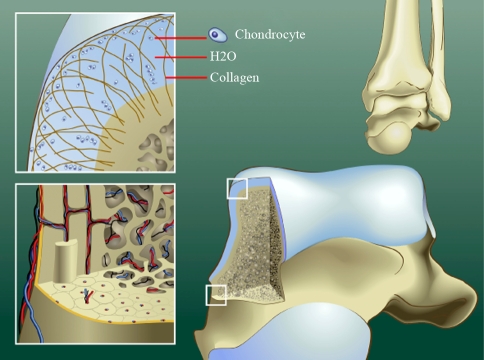
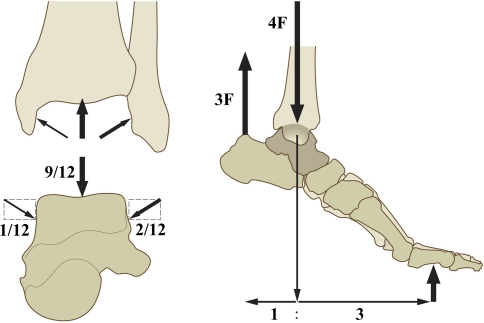
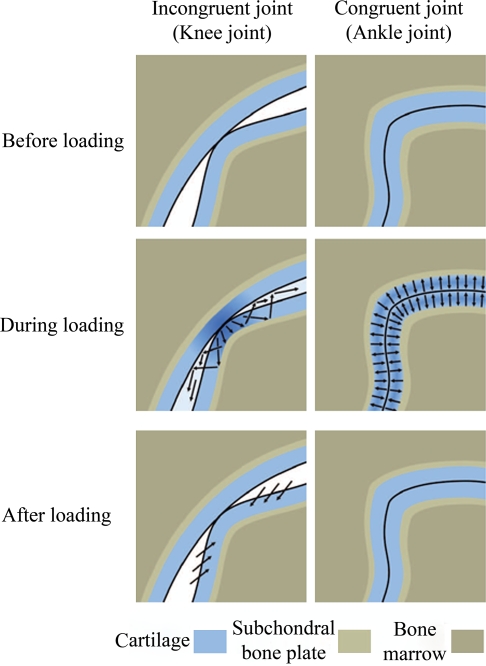
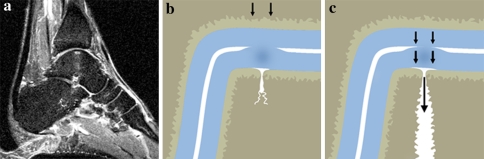
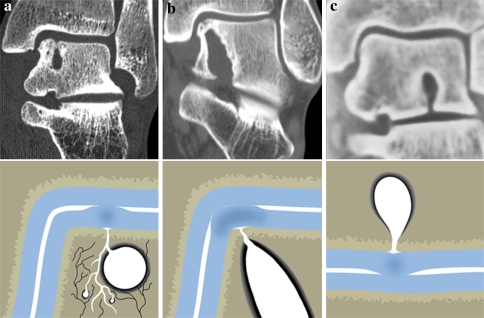
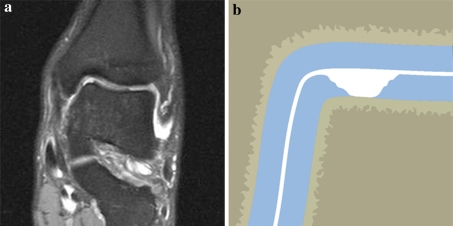
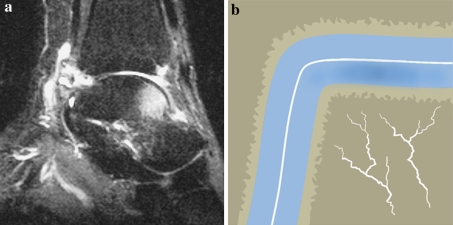
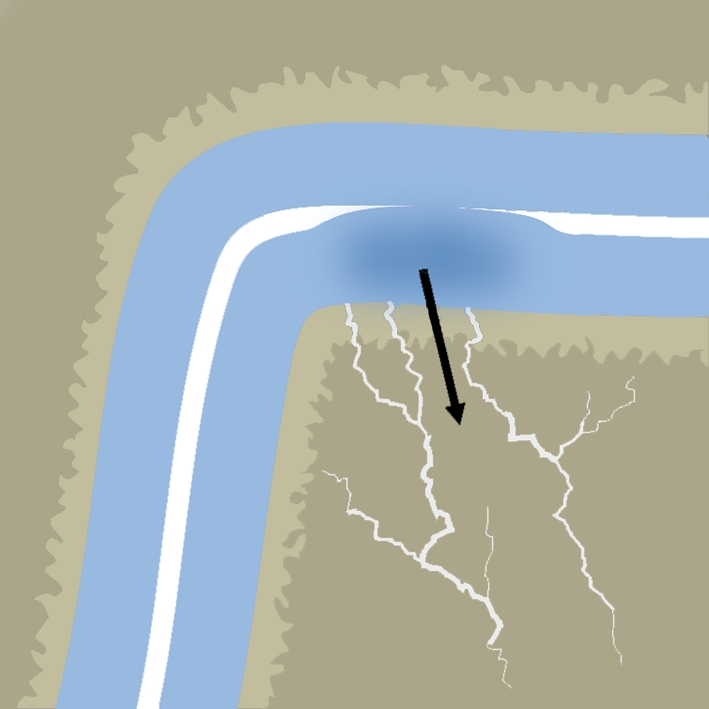
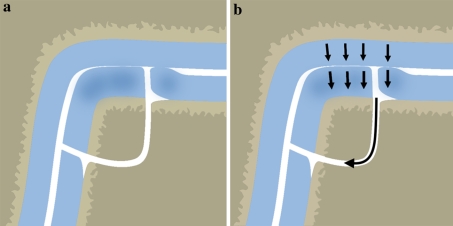
Osteochondral defects of the ankle can either heal and remain asymptomatic or progress to deep ankle pain on weight bearing and formation of subchondral bone cysts. The development of a symptomatic OD depends on various factors, including the damage and insufficient repair of the subchondral bone plate. The ankle joint has a high congruency. During loading, compressed cartilage forces its water into the microfractured subchondral bone, leading to a localized high increased flow and pressure of fluid in the subchondral bone. This will result in local osteolysis and can explain the slow development of a subchondral cyst. The pain does not arise from the cartilage lesion, but is most probably caused by repetitive high fluid pressure during walking, which results in stimulation of the highly innervated subchondral bone underneath the cartilage defect. Understanding the natural history of osteochondral defects could lead to the development of strategies for preventing progressive joint damage.
Figures

References
-
- Anderson DV, Lyne ED. Osteochondritis dissecans of the talus: case report on two family members. J Pediatr Orthop. 1984;4:356–357. - PubMed
-
- Berndt AL, Harty M. Transchondral fractures (osteochondritis dissecans) of the talus. J Bone Joint Surg Am. 1959;41-A:988–1020. - PubMed
-
- Braune W, Fischer O. Die Bewegungen des Kniegelenks nach einer neuen Methode am lebenden Menschen gemessen. Leipzig: S Hirzel; 1891. pp. 75–150.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
