

Proton-beam, intensity-modulated, and/or intraoperative electron radiation therapy combined with aggressive anterior surgical resection for retroperitoneal sarcomas
- PMID: 20151216
- PMCID: PMC2943833
- DOI: 10.1245/s10434-010-0935-1
Proton-beam, intensity-modulated, and/or intraoperative electron radiation therapy combined with aggressive anterior surgical resection for retroperitoneal sarcomas
Abstract
Background: We sought to reduce local recurrence for retroperitoneal sarcomas by using a coordinated strategy of advanced radiation techniques and aggressive en-bloc surgical resection.
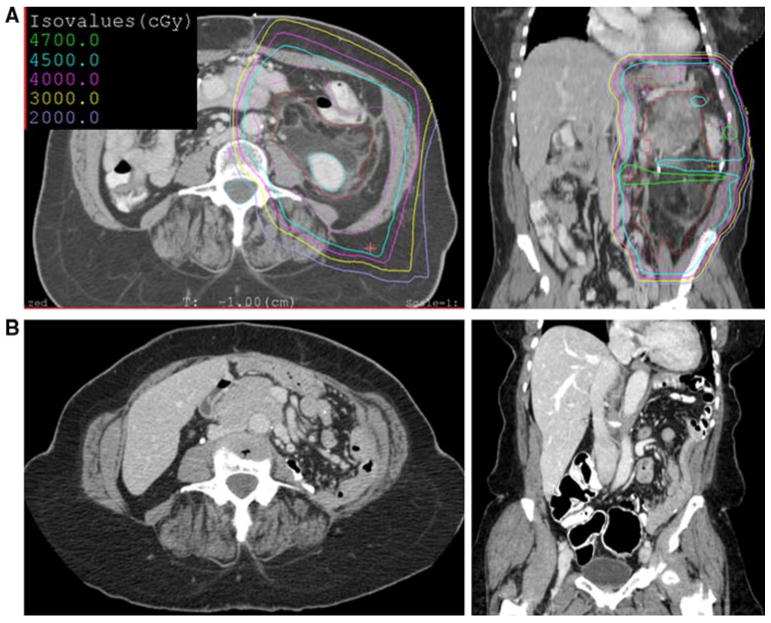
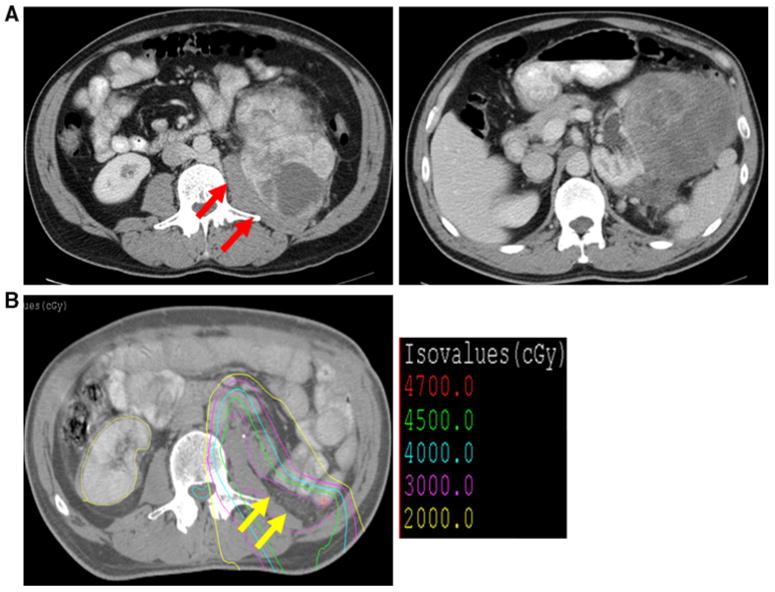
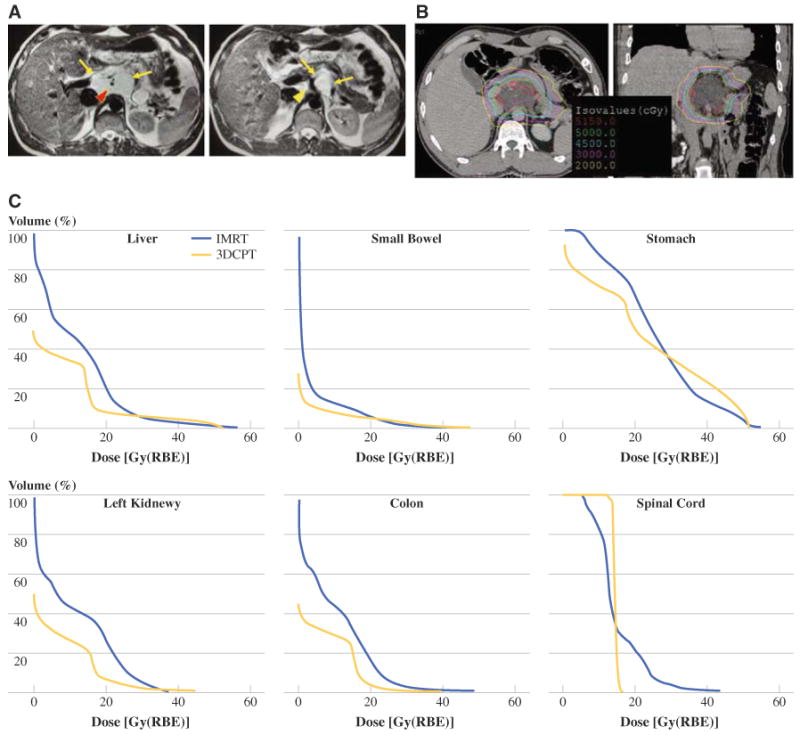
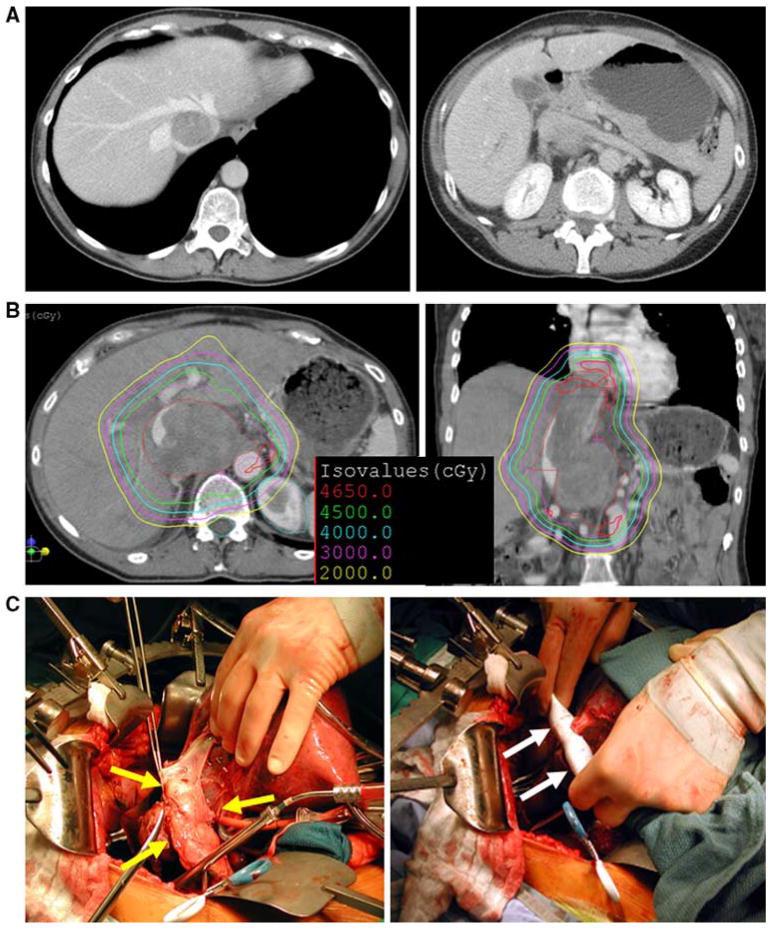
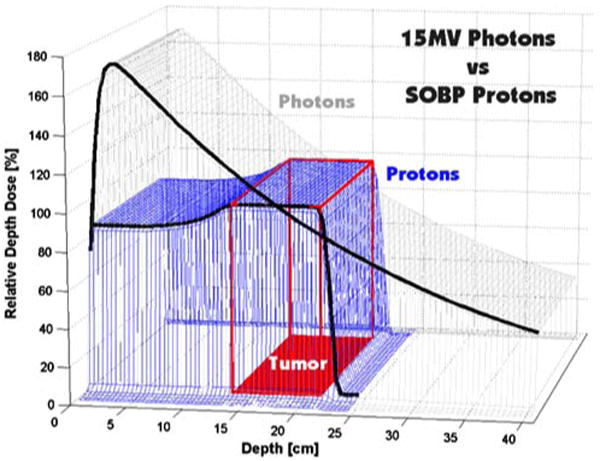
Methods: Proton-beam radiation therapy (PBRT) and/or intensity-modulated radiation therapy (IMRT) were delivered to improve tumor target coverage and spare selected adjacent organs. Surgical resection of tumor and adjacent organs was performed to obtain a disease-free anterior margin. Intraoperative electron radiation therapy (IOERT) was delivered to any close posterior margin.
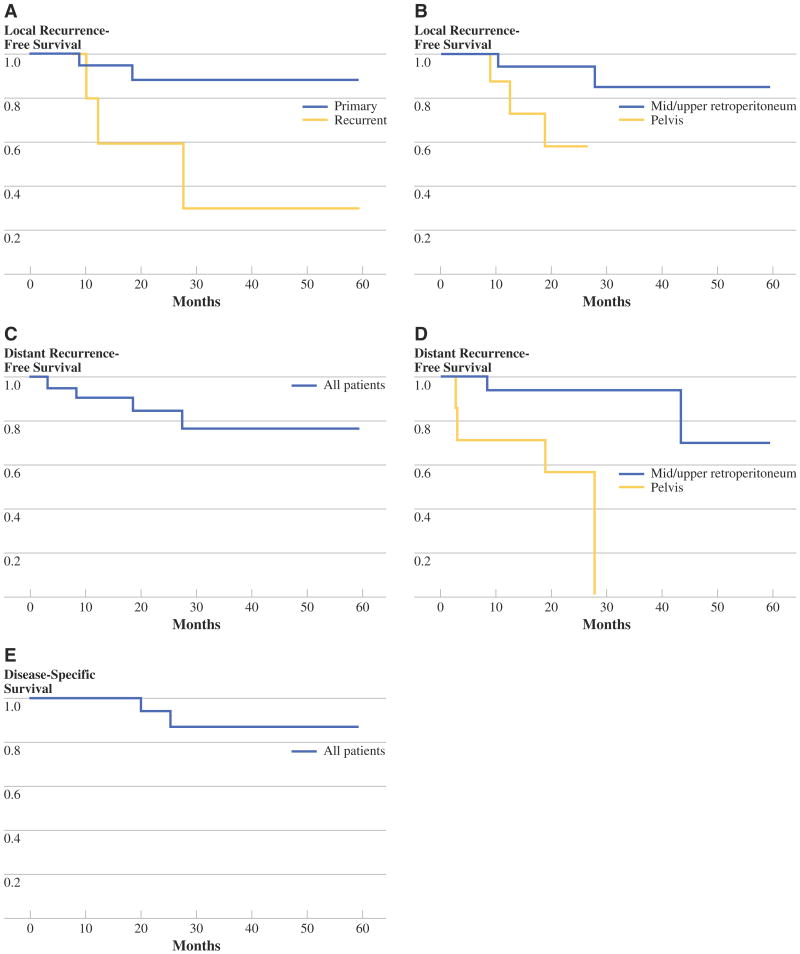
Results: Twenty patients had primary tumors and eight had recurrent tumors. Tumors were large (median size 9.75 cm), primarily liposarcomas and leiomyosarcomas (71%), and were mostly of intermediate or high grade (81%). PBRT and/or IMRT were delivered to all patients, preferably preoperatively (75%), to a median dose of 50 Gy. Surgical resection included up to five adjacent organs, most commonly the colon (n = 7) and kidney (n = 7). Margins were positive for disease, usually posteriorly, in 15 patients (54%). IOERT was delivered to the posterior margin in 12 patients (43%) to a median dose of 11 Gy. Surgical complications occurred in eight patients (28.6%), and radiation-related complications occurred in four patients (14%). After a median follow-up of 33 months, only two patients (10%) with primary disease experienced local recurrence, while three patients (37.5%) with recurrent disease experienced local recurrence.
Conclusions: Aggressive resection of retroperitoneal sarcomas can achieve a disease-negative anterior margin. PBRT and/or IMRT with IOERT may possibly deliver sufficient radiation dose to the posterior margin to control microscopic residual disease. This strategy may minimize radiation-related morbidity and reduce local recurrence, especially in patients with primary disease.
Figures
Similar articles
-
Intensity modulated radiation therapy and surgery for Management of Retroperitoneal Sarcomas: a single-institution experience.Radiat Oncol. 2017 Dec 8;12(1):198. doi: 10.1186/s13014-017-0920-y. Radiat Oncol. 2017. PMID: 29216884 Free PMC article. Clinical Trial.
-
Use of intraoperative electron beam radiotherapy in the management of retroperitoneal soft tissue sarcomas.Int J Radiat Oncol Biol Phys. 2002 Feb 1;52(2):469-75. doi: 10.1016/s0360-3016(01)02595-0. Int J Radiat Oncol Biol Phys. 2002. PMID: 11872294
-
Significance of intraoperative radiation therapy and high cumulative radiation doses in retroperitoneal soft tissue sarcoma.Eur J Surg Oncol. 2020 May;46(5):905-913. doi: 10.1016/j.ejso.2019.12.014. Epub 2019 Dec 17. Eur J Surg Oncol. 2020. PMID: 31892479
-
The role of standard and novel radiotherapy approaches in management of retroperitoneal sarcomas.Eur J Surg Oncol. 2023 Jun;49(6):1111-1114. doi: 10.1016/j.ejso.2022.08.029. Epub 2022 Aug 29. Eur J Surg Oncol. 2023. PMID: 36115783 Review.
-
The importance of surgical margins in retroperitoneal sarcoma.J Surg Oncol. 2016 Mar;113(3):270-6. doi: 10.1002/jso.24135. Epub 2015 Dec 28. J Surg Oncol. 2016. PMID: 26707028 Review.
Cited by
-
The role of radiation in retroperitoneal sarcomas.Curr Treat Options Oncol. 2013 Sep;14(3):425-41. doi: 10.1007/s11864-013-0236-6. Curr Treat Options Oncol. 2013. PMID: 23649911 Free PMC article.
-
Clinical characteristics and management of primary retroperitoneal sarcoma: A literature review.Ann Gastroenterol Surg. 2023 Nov 16;8(1):21-29. doi: 10.1002/ags3.12756. eCollection 2024 Jan. Ann Gastroenterol Surg. 2023. PMID: 38250690 Free PMC article. Review.
-
Definitive Radiotherapy in the Management of Non-Resectable or Residual Retroperitoneal Sarcomas: Institutional Cohort Analysis and Systematic Review.Cancer Control. 2021 Jan-Dec;28:1073274820983028. doi: 10.1177/1073274820983028. Cancer Control. 2021. PMID: 33567904 Free PMC article.
-
Phase 1 trial of preoperative image guided intensity modulated proton radiation therapy with simultaneously integrated boost to the high risk margin for retroperitoneal sarcomas.Adv Radiat Oncol. 2017 Jan 4;2(1):85-93. doi: 10.1016/j.adro.2016.12.003. eCollection 2017 Jan-Mar. Adv Radiat Oncol. 2017. PMID: 28740917 Free PMC article.
-
Comparison of 3D Conformal Proton Therapy, Intensity-Modulated Proton Therapy, and Intensity-Modulated Photon Therapy for Retroperitoneal Sarcoma.Sarcoma. 2022 Mar 19;2022:5540615. doi: 10.1155/2022/5540615. eCollection 2022. Sarcoma. 2022. PMID: 35345672 Free PMC article.
References
-
- Brennan MF, Lewis JL. Diagnosis and management of soft tissue sarcoma. London: Martin Dunitz; 2002.
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2009. CA Cancer J Clin. 2009;59:225–49. - PubMed
-
- Gronchi A, Lo VS, Fiore M, et al. Aggressive surgical policies in a retrospectively reviewed single-institution case series of retroperitoneal soft tissue sarcoma patients. J Clin Oncol. 2009;27:24–30. - PubMed
-
- Bonvalot S, Rivoire M, Castaing M, et al. Primary retroperitoneal sarcomas: a multivariate analysis of surgical factors associated with local control. J Clin Oncol. 2009;27:31–7. - PubMed
-
- Pisters PW. Resection of some—but not all—clinically uninvolved adjacent viscera as part of surgery for retroperitoneal soft tissue sarcomas. J Clin Oncol. 2009;27:6–8. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
