

The right ventricular annular velocity reduction caused by coronary artery bypass graft surgery occurs at the moment of pericardial incision
- PMID: 20152232
- PMCID: PMC2822903
- DOI: 10.1016/j.ahj.2009.11.013
The right ventricular annular velocity reduction caused by coronary artery bypass graft surgery occurs at the moment of pericardial incision
Abstract
Background: Right ventricular (RV) long-axis function is known to be depressed after cardiac surgery, but the mechanism is not known. We hypothesized that intraoperative transesophageal echocardiography could pinpoint the time at which this happens to help narrow the range of plausible mechanisms.
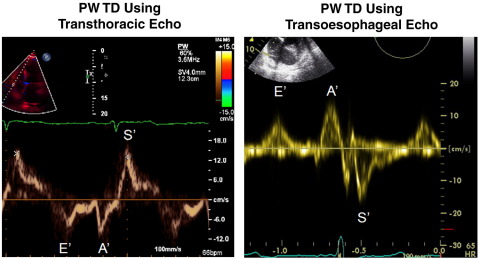
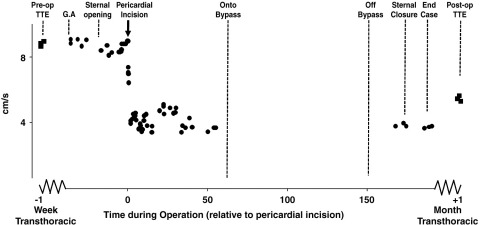
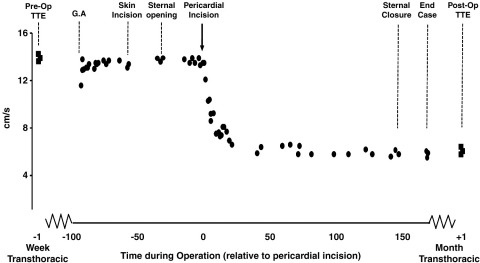
Method: Transthoracic echocardiography was conducted in 33 patients before and after elective coronary artery bypass graft. In an intensively monitored cohort of 9 patients, we also monitored RV function intraoperatively using serial pulsed wave tissue Doppler (PW TD) transesophageal echocardiography.
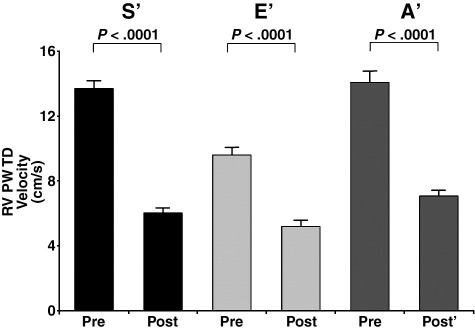
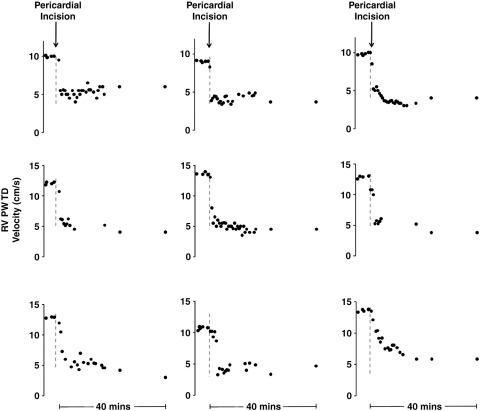
Results: There was no significant difference in myocardial velocities from the onset of the operation up to the beginning of pericardial incision, change in RV PW TD S' velocities 3% +/- 2% (P = not significant). Within the first 3 minutes of opening the pericardium, RV PW TD S' velocities had reduced by 43% +/- 17% (P < .001). At 5 minutes postpericardial incision, 2 minutes later, the velocities had more than halved, by 54% +/- 11% (P < .0001). Velocities thereafter remained depressed throughout the operation, with final intraoperative S' reduction being 61% +/- 11% (P < .0001). One month after surgery, in the full 33-patient cohort, transthoracic echocardiogram data showed a 55% +/- 12% (P < .0001) reduction in RV S' velocities compared with preoperative values.
Conclusions: Minute-by-minute monitoring during cardiac surgery reveals that, virtually, all the losses in RV systolic velocity occurs within the first 3 minutes after pericardial incision. Right ventricular long-axis reduction during coronary bypass surgery results not from cardiopulmonary bypass but rather from pericardial incision.
Copyright (c) 2010 Mosby, Inc. All rights reserved.
Figures
References
-
- Alam M., Hedman A., Norlander R. Right ventricular function before and after an uncomplicated coronary artery bypass graft as assessed by pulsed wave Doppler tissue imaging of the tricuspid annulus. Am Heart J. 2003;146:520–525. - PubMed
-
- Carr-White G.S., Kon M., Koh T.W. Right ventricular function after pulmonary autograft replacement of the aortic valve. Circulation. 1999;100:II–36. - PubMed
-
- Brookes C.I., White P.A., Bishop A.J. Validation of a new intraoperative technique to evaluate load-independent indices of right ventricular performance in patients undergoing cardiac operations. J Thorac Cardiovasc Surg. 1998;116:468–476. - PubMed
-
- Kloner R.A. Clinical evidence for stunned myocardium after CABG. J Card Surg. 1994;9(suppl):397–402. - PubMed
-
- Roberts A.J. Serial assessment of left ventricular performance following CABG. J Thorac Cardiovasc Surg. 1981;81:69–84. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
