

Three-dimensional analysis of maxillary protraction with intermaxillary elastics to miniplates
- PMID: 20152686
- PMCID: PMC2910400
- DOI: 10.1016/j.ajodo.2009.07.009
Three-dimensional analysis of maxillary protraction with intermaxillary elastics to miniplates
Abstract
Introduction: Early Class III treatment with reverse-pull headgear generally results in maxillary skeletal protraction but is frequently also accompanied by unfavorable dentoalveolar effects. An alternative treatment with intermaxillary elastics from a temporary anchorage device might permit equivalent favorable skeletal changes without the unwanted dentoalveolar effects.
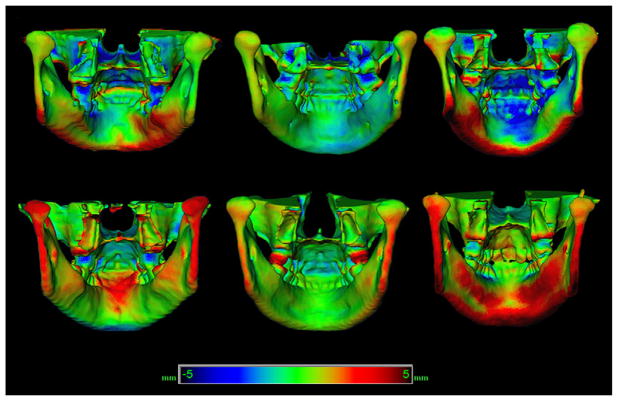
Methods: Six consecutive patients (3 boys, 3 girls; ages, 10-13 years 3 months) with Class III occlusion and maxillary deficiency were treated by using intermaxillary elastics to titanium miniplates. Cone-beam computed tomography scans taken before and after treatment were used to create 3-dimensional volumetric models that were superimposed on nongrowing structures in the anterior cranial base to determine anatomic changes during treatment.
Results: The effect of the intermaxillary elastic forces was throughout the nasomaxillary structures. All 6 patients showed improvements in the skeletal relationship, primarily through maxillary advancement with little effect on the dentoalveolar units or change in mandibular position.
Conclusions: The use of intermaxillary forces applied to temporary anchorage devices appears to be a promising treatment method.
Conflict of interest statement
The authors report no commercial, proprietary, or financial interest in the products or companies described in this article.
Figures









Similar articles
-
Class III Treatment with Skeletal and Dental Anchorage: A Review of Comparative Effects.Biomed Res Int. 2018 Jul 2;2018:7946019. doi: 10.1155/2018/7946019. eCollection 2018. Biomed Res Int. 2018. PMID: 30057910 Free PMC article. Review.
-
Three-dimensional assessment of maxillary changes associated with bone anchored maxillary protraction.Am J Orthod Dentofacial Orthop. 2011 Dec;140(6):790-8. doi: 10.1016/j.ajodo.2011.04.025. Am J Orthod Dentofacial Orthop. 2011. PMID: 22133943 Free PMC article. Clinical Trial.
-
Three-dimensional assessment of mandibular and glenoid fossa changes after bone-anchored Class III intermaxillary traction.Am J Orthod Dentofacial Orthop. 2012 Jul;142(1):25-31. doi: 10.1016/j.ajodo.2012.01.017. Am J Orthod Dentofacial Orthop. 2012. PMID: 22748987 Free PMC article.
-
Use of intermaxillary forces in early treatment of maxillary deficient class III patients: results of a case series.J Craniomaxillofac Surg. 2012 Dec;40(8):e350-4. doi: 10.1016/j.jcms.2012.01.019. Epub 2012 Mar 14. J Craniomaxillofac Surg. 2012. PMID: 22421469
-
Maxillary protraction at early ages. The revolution of new bone anchorage appliances.J Clin Pediatr Dent. 2012 Winter;37(2):219-29. doi: 10.17796/jcpd.37.2.q0k770403v443053. J Clin Pediatr Dent. 2012. PMID: 23534334 Review.
Cited by
-
The efficacy of maxillary protraction protocols with the micro-implant-assisted rapid palatal expander (MARPE) and the novel N2 mini-implant-a finite element study.Prog Orthod. 2015;16:16. doi: 10.1186/s40510-015-0083-z. Epub 2015 Jun 4. Prog Orthod. 2015. PMID: 26061987 Free PMC article.
-
Three-dimensional evaluation of soft tissue changes in the orofacial region after tooth-borne and bone-borne surgically assisted rapid maxillary expansion.Clin Oral Investig. 2013 Dec;17(9):2017-24. doi: 10.1007/s00784-013-0927-1. Epub 2013 Feb 2. Clin Oral Investig. 2013. PMID: 23377777
-
Class III Treatment with Skeletal and Dental Anchorage: A Review of Comparative Effects.Biomed Res Int. 2018 Jul 2;2018:7946019. doi: 10.1155/2018/7946019. eCollection 2018. Biomed Res Int. 2018. PMID: 30057910 Free PMC article. Review.
-
Class III correction using an inter-arch spring-loaded module.Prog Orthod. 2014 May 2;15(1):32. doi: 10.1186/s40510-014-0032-2. Prog Orthod. 2014. PMID: 24934153 Free PMC article.
-
Cone-Beam Computed Tomography in Orthodontics.Dent J (Basel). 2019 Sep 2;7(3):89. doi: 10.3390/dj7030089. Dent J (Basel). 2019. PMID: 31480667 Free PMC article. Review.
References
-
- Gallagher RW, Miranda F, Buschang PH. Maxillary protraction: treatment and posttreatment effects. Am J Orthod Dentofacial Orthop. 1998;113:612–9. - PubMed
-
- Turley PK. Managing the developing Class III malocclusion with palatal expansion and facemask therapy. Am J Orthod Dentofacial Orthop. 2002;122:349–52. - PubMed
-
- Baik HS. Clinical results of the maxillary protraction in Korean children. Am J Orthod Dentofacial Orthop. 1995;108:583–92. - PubMed
-
- Cha KS. Skeletal changes of maxillary protraction in patients exhibiting skeletal Class III malocclusion: a comparison of three skeletal maturation groups. Angle Orthod. 2003;73:26–35. - PubMed
-
- Ishii H, Morita S, Takeuchi Y, Nakamura S. Treatment effect of combined maxillary protraction and chincap appliance in severe skeletal Class III cases. Am J Orthod Dentofacial Orthop. 1987;92:304–12. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
