

J wave syndromes
- PMID: 20153265
- PMCID: PMC2843811
- DOI: 10.1016/j.hrthm.2009.12.006
J wave syndromes
Abstract
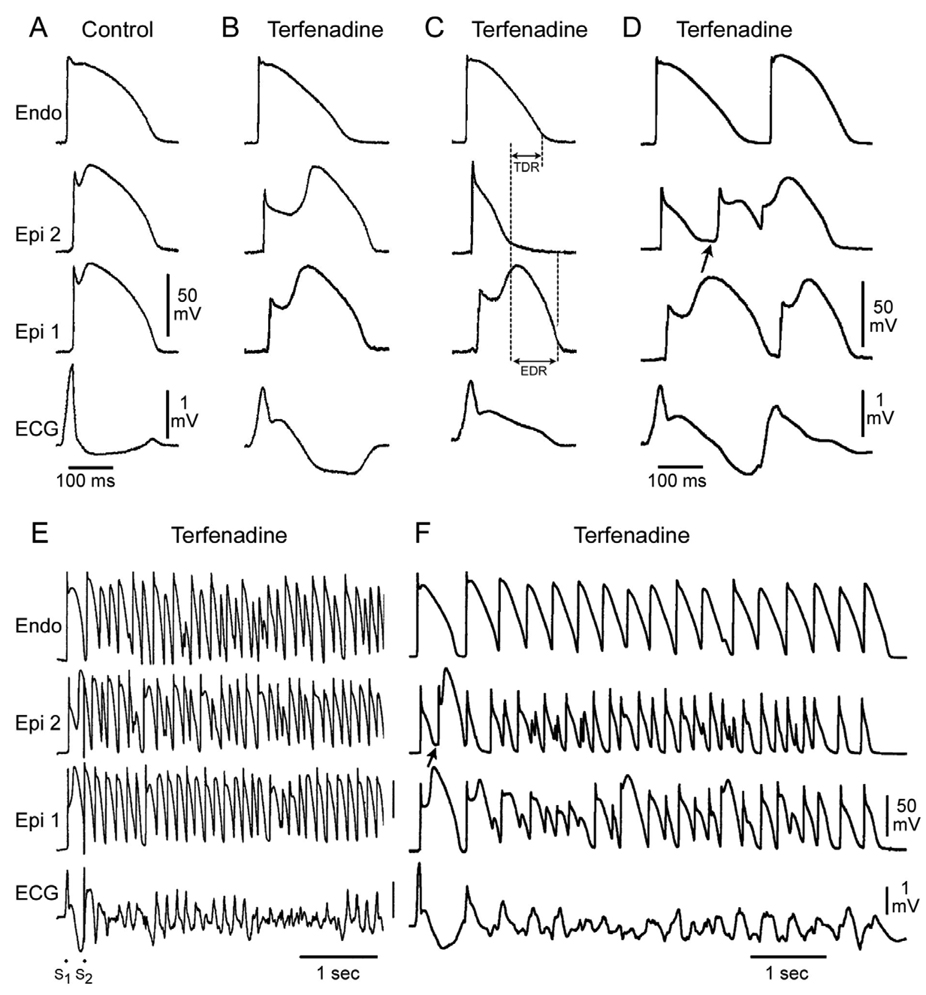
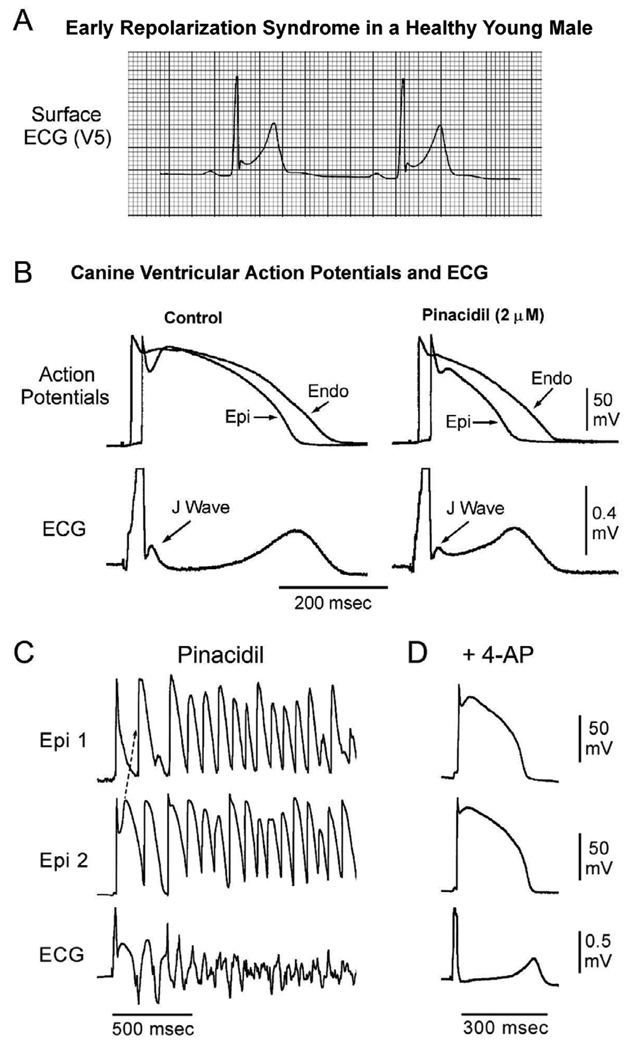
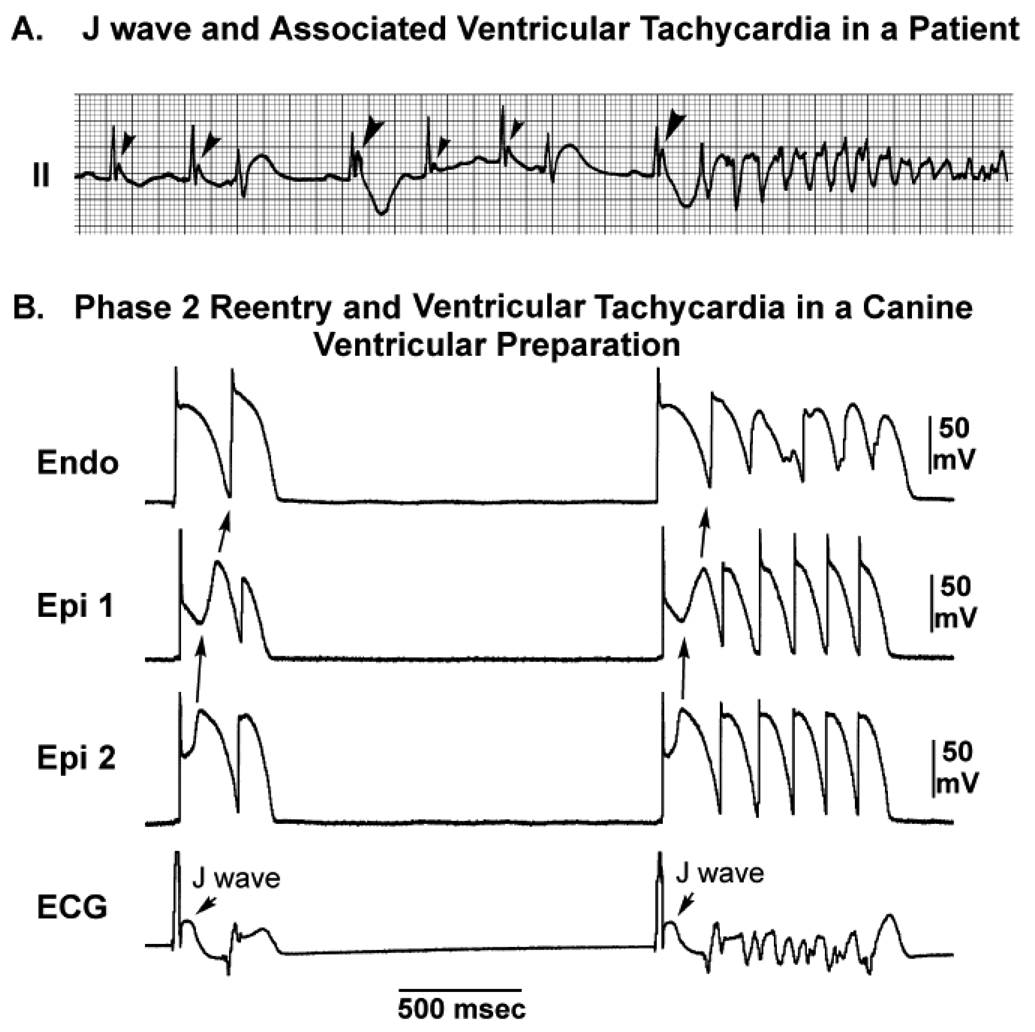
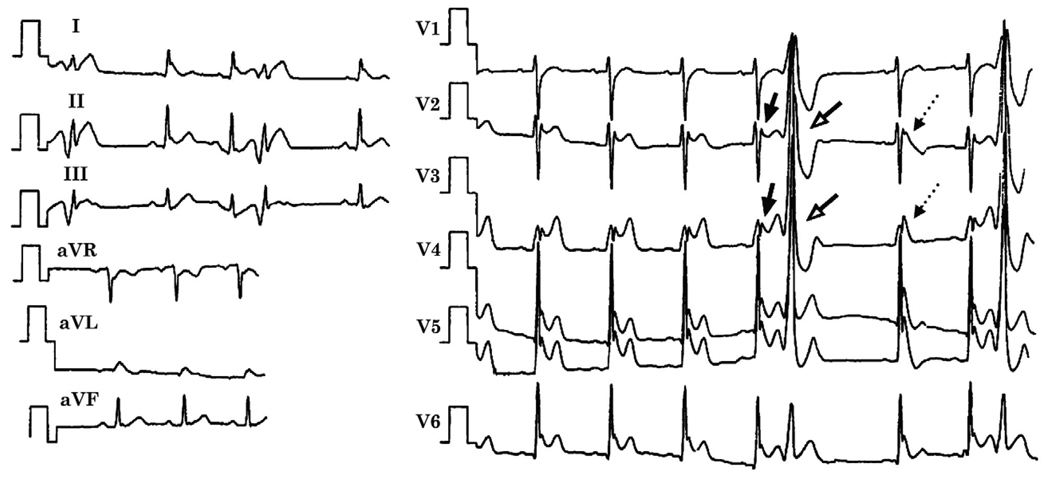
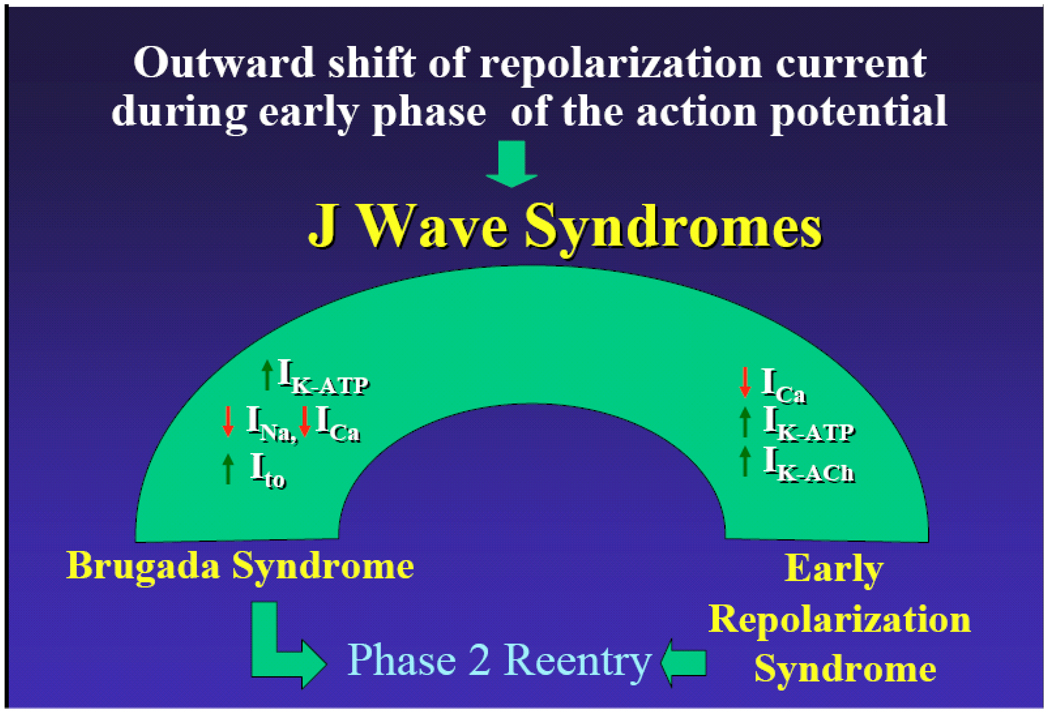
The J wave, also referred to as an Osborn wave, is a deflection immediately following the QRS complex of the surface ECG. When partially buried in the R wave, the J wave appears as J-point elevation or ST-segment elevation. Several lines of evidence have suggested that arrhythmias associated with an early repolarization pattern in the inferior or mid to lateral precordial leads, Brugada syndrome, or arrhythmias associated with hypothermia and the acute phase of ST-segment elevation myocardial infarction are mechanistically linked to abnormalities in the manifestation of the transient outward current (I(to))-mediated J wave. Although Brugada syndrome and early repolarization syndrome differ with respect to the magnitude and lead location of abnormal J-wave manifestation, they can be considered to represent a continuous spectrum of phenotypic expression that we propose be termed J-wave syndromes. This review summarizes our current state of knowledge concerning J-wave syndromes, bridging basic and clinical aspects. We propose to divide early repolarization syndrome into three subtypes: type 1, which displays an early repolarization pattern predominantly in the lateral precordial leads, is prevalent among healthy male athletes and is rarely seen in ventricular fibrillation survivors; type 2, which displays an early repolarization pattern predominantly in the inferior or inferolateral leads, is associated with a higher level of risk; and type 3, which displays an early repolarization pattern globally in the inferior, lateral, and right precordial leads, is associated with the highest level of risk for development of malignant arrhythmias and is often associated with ventricular fibrillation storms.
Copyright 2010 Heart Rhythm Society. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures


References
-
- Osborn JJ. Experimental hypothermia: respiratory and blood pH changes in relation to cardiac function. Am J Physiol. 1953;175:389–398. - PubMed
-
- Yan GX, Antzelevitch C. Cellular basis for the electrocardiographic J wave. Circulation. 1996;93:372–379. - PubMed
-
- Gussak I, Antzelevitch C. Early repolarization syndrome: clinical characteristics and possible cellular and ionic mechanisms. J Electrocardiol. 2000;33:299–309. - PubMed
-
- Yan GX, Yao QH, Wang DQ, Cui CC. Electrocardiographic J wave and J wave syndromes. Chin J Cardiac Arrhyth. 2004;8:360–365.
-
- Shu J, Zhu T, Yang L, Cui C, Yan GX. ST-segment elevation in the early repolarization syndrome, idiopathic ventricular fibrillation, and the Brugada syndrome: cellular and clinical linkage. J Electrocardiol. 2005;38:26–32. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
