

A critical assessment of the out-of-hospital trauma triage guidelines for physiologic abnormality
- PMID: 20154558
- PMCID: PMC3785297
- DOI: 10.1097/TA.0b013e3181ae20c9
A critical assessment of the out-of-hospital trauma triage guidelines for physiologic abnormality
Abstract
Background: It remains unclear whether the American College of Surgeons Committee on Trauma (ACSCOT) "step 1" field physiologic criteria could be further restricted without substantially sacrificing sensitivity. We assessed whether more restrictive physiologic criteria would improve the specificity of this triage step without missing high-risk patients.
Methods: We analyzed an out-of-hospital, consecutive patient, prospective cohort of injured adults >or=15 years collected from December 1, 2005, to February 28, 2007, by 237 emergency medical service agencies transporting to 207 acute care hospitals in 11 sites across the United States and Canada. Patients were included based on ACSCOT field decision scheme physiologic criteria systolic blood pressure <or=90, respiratory rate <10 or >29 breaths/min, Glasgow Coma Scale score <or=12, or field intubation. Seven field physiologic variables and four additional demographic and mechanism variables were included in the analysis. The composite outcome was mortality (field or in-hospital) or hospital length of stay >2 days.
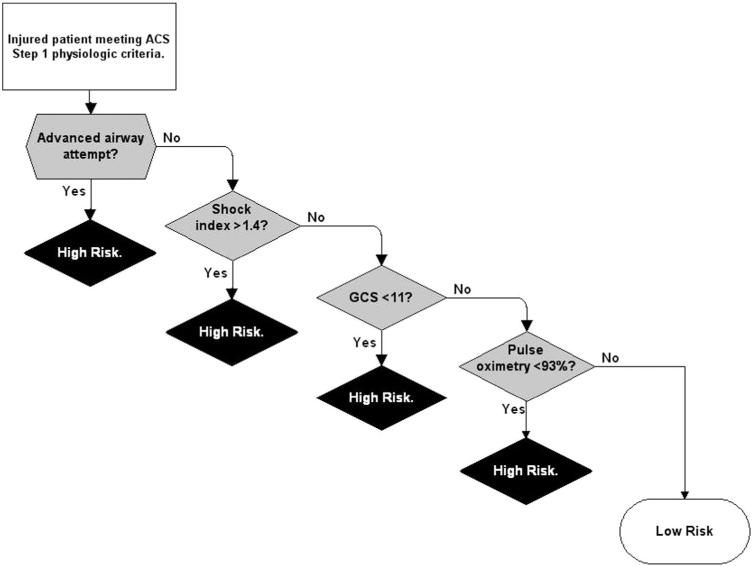
Results: Of 7,127 injured persons, 6,259 had complete outcome information and were included in the analysis. There were 3,631 (58.0%) persons with death or LOS >2 days. Using only physiologic measures, the derived rule included advanced airway intervention, shock index >1.4, Glasgow Coma Scale <11, and pulse oximetry <93%. Rule validation demonstrated sensitivity 72% (95% confidence interval: 70%-74%) and specificity 69% (95% confidence interval: 67%-72%). Inclusion of demographic and mechanism variables did not significantly improve performance measures.
Conclusions: We were unable to omit or further restrict any ACSCOT step 1 physiologic measures in a decision rule practical for field use without missing high-risk trauma patients.
Figures
References
-
- Mackersie RC. History of trauma field triage development and the American College of Surgeons criteria. Prehosp Emerg Care. 2006;10:287–294. - PubMed
-
- Committee on Trauma . Resources for Optimal Care of the Injured Patient. American College of Surgeons; Chicago, IL: 2006.
-
- Cottington EM, Young JC, Shufflebarger CM, Kyes F, Peterson FV, Jr, Diamond DL. The utility of physiologic status, injury site, and injury mechanism in identifying patients with major trauma. J Trauma. 1988;28:305–311. - PubMed
-
- Esposito TJ, Offner PJ, Jurkovich GJ, Griffith J, Maier RV. Do prehospital trauma center triage criteria identify major trauma victims? Arch Surg. 1995;130:171–176. - PubMed
-
- Kane G, Engelhardt R, Celentano J, et al. Empirical development and evaluation of out of hospital trauma triage instruments. J Trauma. 1985;25:482–489. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 HL077866/HL/NHLBI NIH HHS/United States
- U01 HL077871/HL/NHLBI NIH HHS/United States
- CAPMC/ CIHR/Canada
- HL077867/HL/NHLBI NIH HHS/United States
- U54 MD007584/MD/NIMHD NIH HHS/United States
- 5U01 HL077863/HL/NHLBI NIH HHS/United States
- U01 HL077881/HL/NHLBI NIH HHS/United States
- HL077873/HL/NHLBI NIH HHS/United States
- U01 HL077872/HL/NHLBI NIH HHS/United States
- HL077871/HL/NHLBI NIH HHS/United States
- HL077881/HL/NHLBI NIH HHS/United States
- HL077908/HL/NHLBI NIH HHS/United States
- HL077877/HL/NHLBI NIH HHS/United States
- U01 HL077885/HL/NHLBI NIH HHS/United States
- U01 HL077863/HL/NHLBI NIH HHS/United States
- U01 HL077908/HL/NHLBI NIH HHS/United States
- HL077872/HL/NHLBI NIH HHS/United States
- HL077866/HL/NHLBI NIH HHS/United States
- U01 HL077873/HL/NHLBI NIH HHS/United States
- U01 HL077867/HL/NHLBI NIH HHS/United States
- HL077885/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
