

Examining the promise of HIV elimination by 'test and treat' in hyperendemic settings
- PMID: 20154580
- PMCID: PMC2852517
- DOI: 10.1097/QAD.0b013e32833433fe
Examining the promise of HIV elimination by 'test and treat' in hyperendemic settings
Abstract
Background: It has been suggested that a new strategy for HIV prevention, 'Universal Test and Treat', whereby everyone is tested for HIV once a year and treated immediately with antiretroviral therapy (ART) if they are infected, could 'eliminate' the epidemic and reduce ART costs in the long term.
Methods: We investigated the impact of test-and-treat interventions under a variety of assumptions about the epidemic using a deterministic mathematical model.
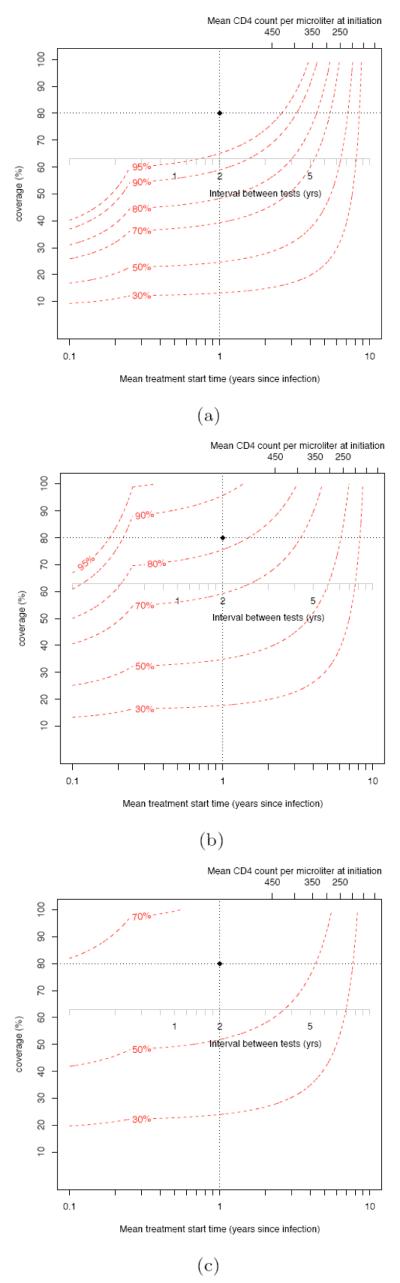
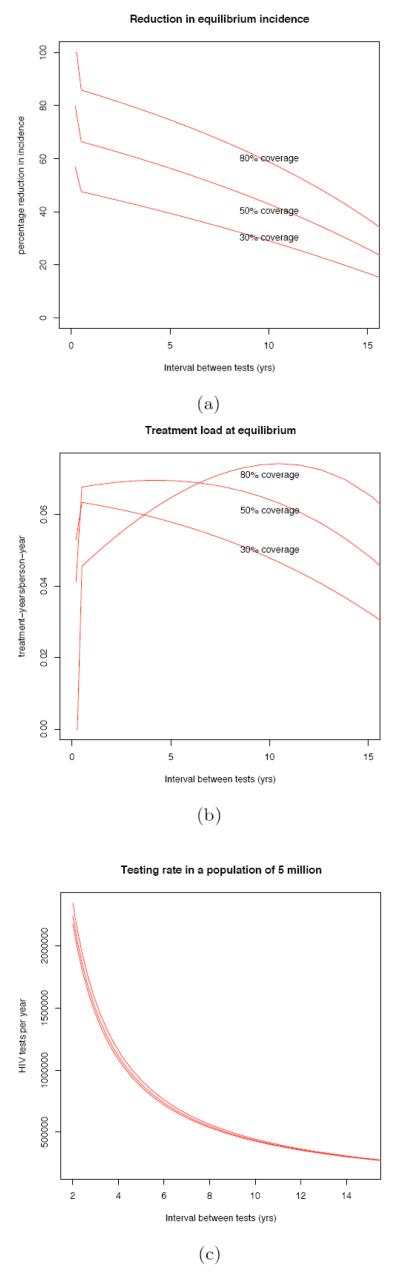
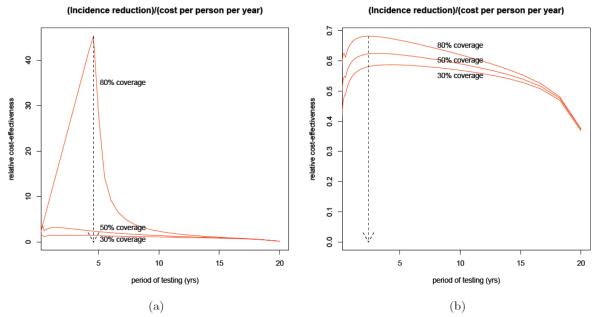
Results: Our model shows that such an intervention can substantially reduce HIV transmission, but that impact depends crucially on the epidemiological context; in some situations, less aggressive interventions achieve the same results, whereas in others, the proposed intervention reduces HIV by much less. It follows that testing every year and treating immediately is not necessarily the most cost-efficient strategy. We also show that a test-and-treat intervention that does not reach full implementation or coverage could, perversely, increase long-term ART costs.
Conclusion: Interventions that prevent new infections through ART scale-up may hold substantial promise. However, as plans move forward, careful consideration should be given to the nature of the epidemic and the potential for perverse outcomes.
Figures
References
-
- UNAIDS . Report on the global AIDS epidemic. UNAIDS; Geneva: 2008. http://www.unaids.org/en/KnowledgeCentre/HIVData/GlobalReport/2008/2008_....
-
- WHO. UNAIDS. UNICEF . Towards Universal Access: Scaling up priority HIV/AIDS interventions in the health sector Progress Report. Geneva: 2008. available from http://www.who.int/hiv/pub/towards_universal_access_report_2008.pdf.
-
- Piot P, Bartos M, Larson H, Zewdie D, Mane P. Coming to terms with complexity: a call to action for HIV prevention. Lancet. 2008;372:845–859. - PubMed
-
- Sherr L, Lopman B, Kakowa M, Dube S, Chawira G, Nyamukapa C, et al. Voluntary counselling and testing: uptake, impact on sexual behaviour, and HIV incidence in a rural Zimbabwean cohort. AIDS. 2007;21:851–860. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
