

Uncoupling between insulin and release of a D-chiro-inositol-containing inositolphosphoglycan mediator of insulin action in obese women With polycystic ovary syndrome
- PMID: 20156067
- PMCID: PMC3140116
- DOI: 10.1089/met.2009.0052
Uncoupling between insulin and release of a D-chiro-inositol-containing inositolphosphoglycan mediator of insulin action in obese women With polycystic ovary syndrome
Abstract
Background: Obese women with polycystic ovary syndrome (PCOS) manifest impaired insulin-stimulated release of a d-chiro-inositol-containing inositolphosphoglycan (DCI-IPG) insulin mediator during oral glucose tolerance testing (OGTT), which appears to be restored by the administration of metformin. This suggests that either obesity or PCOS is associated with a defect in the coupling of the stimulation of the insulin receptor by insulin to the release of the DCI-IPG mediator. The objective of this study was to compare the release of bioactive DCI-IPG between normal nonobese women and obese PCOS women during stimulation with two different concentrations of insulin when glucose levels are clamped.
Methods: We performed a cross-sectional case-control study at the clinical research center of an academic medical center. A two-step euglycemic-hyperinsulinemic clamp was carried out in 8 nonobese normal and 8 obese PCOS women, during which DCI-IPG bioactivity was monitored.
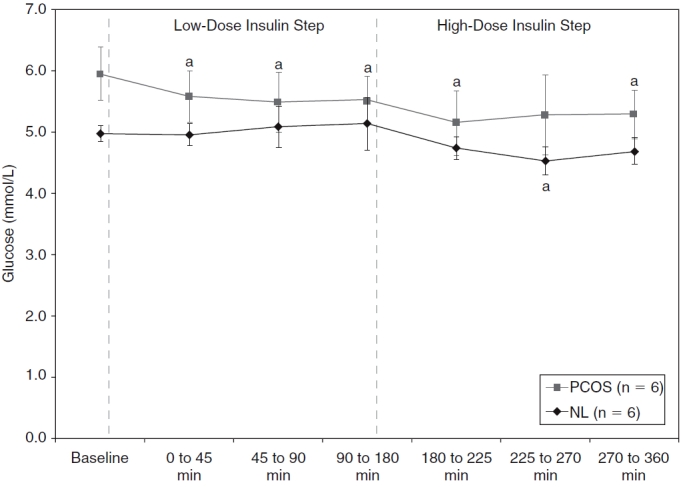
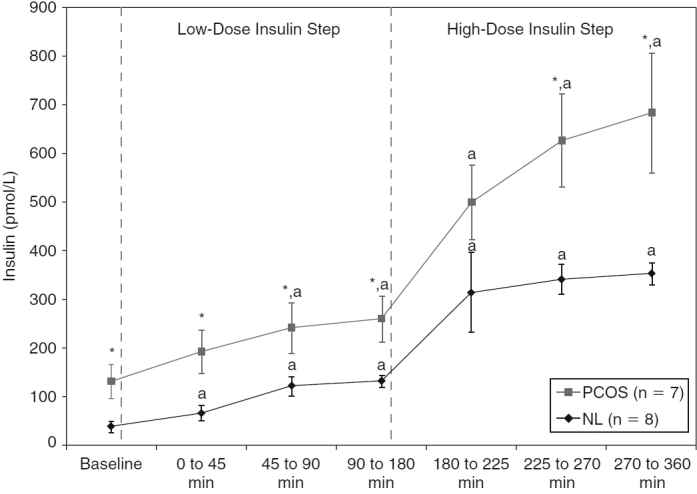
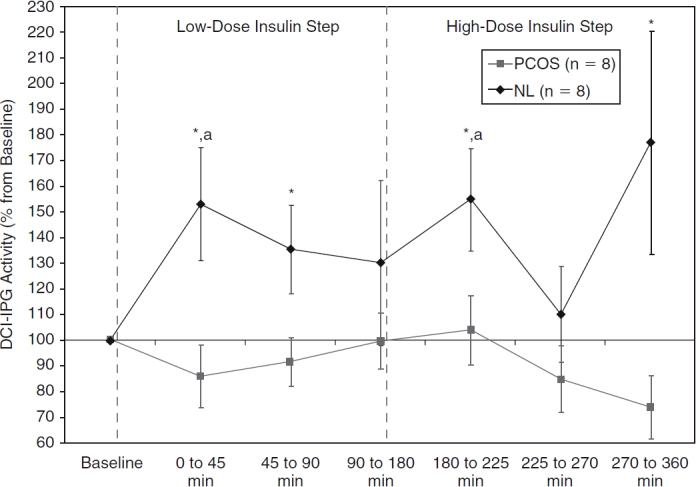
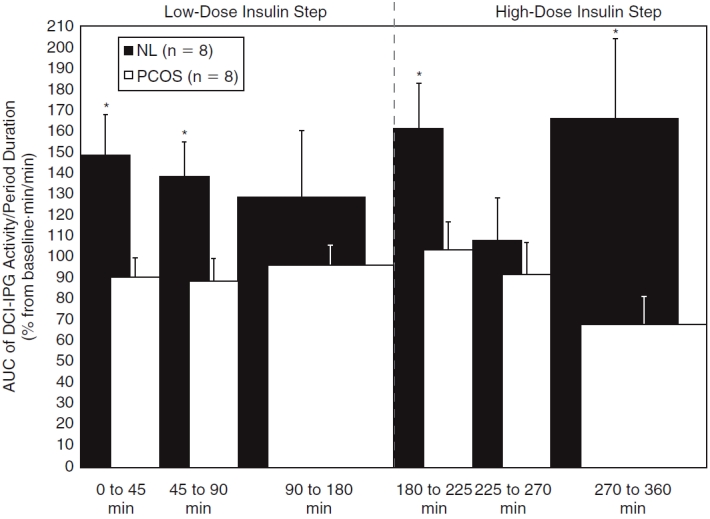
Results: At baseline, PCOS women were significantly more obese, hyperinsulinemic, and insulin resistant than the controls. During the clamp studies, DCI-IPG bioactivity increased significantly over the first 45 min of the low-insulin step of the clamp in normal nonobese women (P = 0.046) and then decreased to baseline levels; DCI-IPG increased again after initiation of the high-insulin step (P = 0.029). Despite higher insulin levels during the clamp in PCOS women, DCI-IPG bioactivity remained flat throughout both insulin steps and was thus significantly lower than in controls during the initial periods of both steps.
Conclusions: The coupling between insulin action and the release of the DCI-IPG mediator is selectively impaired in obese PCOS women, which may contribute to the insulin resistance in these women.
Figures
Similar articles
-
Pioglitazone Therapy Increases Insulin-Stimulated Release of d-Chiro-Inositol-Containing Inositolphosphoglycan Mediator in Women with Polycystic Ovary Syndrome.Metab Syndr Relat Disord. 2016 Oct;14(8):391-396. doi: 10.1089/met.2016.0009. Epub 2016 Mar 30. Metab Syndr Relat Disord. 2016. PMID: 27028341 Free PMC article. Clinical Trial.
-
Metformin therapy increases insulin-stimulated release of D-chiro-inositol-containing inositolphosphoglycan mediator in women with polycystic ovary syndrome.J Clin Endocrinol Metab. 2004 Jan;89(1):242-9. doi: 10.1210/jc.2003-030437. J Clin Endocrinol Metab. 2004. PMID: 14715857 Clinical Trial.
-
Insulin-stimulated release of D-chiro-inositol-containing inositolphosphoglycan mediator correlates with insulin sensitivity in women with polycystic ovary syndrome.Metabolism. 2008 Oct;57(10):1390-7. doi: 10.1016/j.metabol.2008.05.008. Metabolism. 2008. PMID: 18803944 Free PMC article. Clinical Trial.
-
Role of inositolphosphoglycan mediators of insulin action in the polycystic ovary syndrome.J Pediatr Endocrinol Metab. 2000;13 Suppl 5:1295-8. J Pediatr Endocrinol Metab. 2000. PMID: 11117673 Review.
-
D-Chiro-inositol and its significance in polycystic ovary syndrome: a systematic review.Gynecol Endocrinol. 2011 Apr;27(4):256-62. doi: 10.3109/09513590.2010.538099. Epub 2010 Dec 10. Gynecol Endocrinol. 2011. PMID: 21142777
Cited by
-
New Insights into the Activities of D-Chiro-Inositol: A Narrative Review.Biomedicines. 2021 Oct 2;9(10):1378. doi: 10.3390/biomedicines9101378. Biomedicines. 2021. PMID: 34680494 Free PMC article. Review.
-
Interventions to prevent women from developing gestational diabetes mellitus: an overview of Cochrane Reviews.Cochrane Database Syst Rev. 2020 Jun 11;6(6):CD012394. doi: 10.1002/14651858.CD012394.pub3. Cochrane Database Syst Rev. 2020. PMID: 32526091 Free PMC article.
-
Pioglitazone Therapy Increases Insulin-Stimulated Release of d-Chiro-Inositol-Containing Inositolphosphoglycan Mediator in Women with Polycystic Ovary Syndrome.Metab Syndr Relat Disord. 2016 Oct;14(8):391-396. doi: 10.1089/met.2016.0009. Epub 2016 Mar 30. Metab Syndr Relat Disord. 2016. PMID: 27028341 Free PMC article. Clinical Trial.
-
Nutrition as Prevention Factor of Gestational Diabetes Mellitus: A Narrative Review.Nutrients. 2021 Oct 26;13(11):3787. doi: 10.3390/nu13113787. Nutrients. 2021. PMID: 34836042 Free PMC article. Review.
-
What is new in the landscape of insulin-sensitizing agents for polycystic ovary syndrome treatment.Ther Adv Reprod Health. 2020 Feb 27;14:2633494120908709. doi: 10.1177/2633494120908709. eCollection 2020 Jan-Dec. Ther Adv Reprod Health. 2020. PMID: 32435760 Free PMC article. Review.
References
-
- Allen SE, Potter HD, Azziz R. Prevalence of hyperandrogenemia among nonhirsute oligo-ovulatory women. Fertil Steril. 1997;67:569–572. - PubMed
-
- Knochenhauer ES, Key TJ, Kahsar-Miller M, Waggoner W, Boots LR, Azziz R. Prevalence of the polycystic ovary syndrome in unselected black and white women of the southeastern United States: A prospective study. J Clin Endocrinol Metab. 1998;83:3078–3082. - PubMed
-
- Baillargeon JP, Iuorno MJ, Nestler JE. Insulin sensitizers for polycystic ovary syndrome. Clin Obstet Gynecol. 2003;46:325–340. - PubMed
-
- Cattrall FR, Healy DL. Long-term metabolic, cardiovascular and neoplastic risks with polycystic ovary syndrome. Best Pract Res Clin Obstet Gynecol. 2004;18:803–812. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical