

Predicting adult body mass index-specific metabolic risk from childhood
- PMID: 20156071
- PMCID: PMC3035100
- DOI: 10.1089/met.2009.0063
Predicting adult body mass index-specific metabolic risk from childhood
Abstract
Background: Metabolic risk varies within adult body mass index (BMI) categories; however, the development of BMI-specific metabolic risk from childhood is unknown.
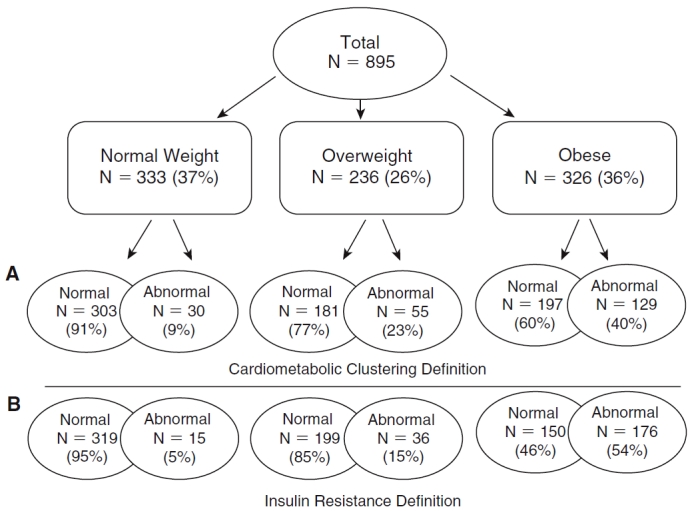
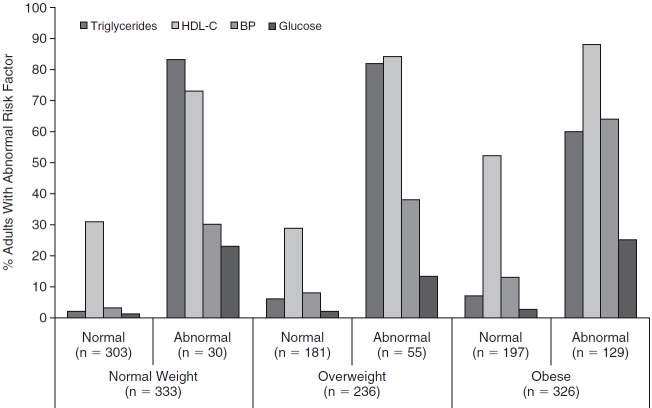
Methods: The sample included 895 adults (20-38 years of age; 43% male, 34% black) from the Bogalusa Heart Study (1995-2002), who had been measured as children (5-18 years of age) in 1981-1982. Adult metabolic risk was assessed using two definitions: Cardiometabolic risk factor clustering (RFC) included two or more abnormal risk factors [blood pressure, high-density lipoprotein cholesterol (HDL-C), triglycerides, and fasting glucose] and insulin resistance (IR), comprising the top quartile of the homeostasis model of insulin resistance (HOMA-IR) distribution. Logistic regression, within BMI categories, was used to predict adult metabolic risk from childhood mean arterial pressure (MAP), HDL-C, low-density lipoprotein cholesterol (LDL-C), glucose, and triglycerides. Covariates included childhood age, race, sex, adult BMI, and length of follow-up.
Results: The prevalence of the adult abnormal metabolic risk profile varied by definitions of metabolic risk (normal weight, 5%-9%; overweight, 15%-23%; and obese, 40%-53%). The adult abnormal profile was associated with higher childhood LDL-C [IR, odds ratio (OR), 1.95; 95% confidence interval (CI), 1.06-3.58) and insulin (IR, OR, 1.69; CI, 1.10-2.58) in normal-weight adults; lower childhood HDL-C in overweight adults (RFC, OR, 0.61; CI, 0.40-0.94); and higher childhood MAP (RFC, OR, 1.75; CI, 1.24-2.47) and glucose (IR, OR,1.38; CI, 1.06-1.81) in obese adults.
Conclusions: Some childhood metabolic risk factors are moderately associated with adult BMI-specific metabolic risk profiles. The ability to identify children with high future adult cardiovascular risk may initiate early treatment options.
Figures
References
-
- Conus F, Rabasa-Lhoret R, Peronnet F. Characteristics of metabolically obese normal-weight (MONW) subjects. Appl Physiol Nutr Metab. 2007;32:4–12. - PubMed
-
- Ruderman NB, Schneider SH, Berchtold P. The “metabolically-obese,” normal-weight individual. Am J Clin Nutr. 1981;34:1617–1621. - PubMed
-
- Tanaka S, Togashi K, Rankinen T, Perusse L, Leon AS, Rao DC, Skinner JS, Wilmore JH, Bouchard C. Is adiposity at normal body weight relevant for cardiovascular disease risk? Int J Obes Relat Metab Disord. 2002;26:176–183. - PubMed
-
- Meigs JB, Wilson PW, Fox CS, Vasan RS, Nathan DM, Sullivan LM, D'Agostino RB. Body mass index, metabolic syndrome, and risk of type 2 diabetes or cardiovascular disease. J Clin Endocrinol Metab. 2006;91:2906–2912. - PubMed
-
- Karelis AD, Brochu M, Rabasa-Lhoret R. Can we identify metabolically healthy but obese individuals (MHO)? Diabetes Metab. 2004;30:569–572. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical