

Endothelial dysfunction in obese non-hypertensive children without evidence of sleep disordered breathing
- PMID: 20156343
- PMCID: PMC2829007
- DOI: 10.1186/1471-2431-10-8
Endothelial dysfunction in obese non-hypertensive children without evidence of sleep disordered breathing
Abstract
Background: Endothelial dysfunction is a complication of both obesity and obstructive sleep apnea syndrome (OSAS), the latter being highly prevalent among obese children. It is unknown whether obesity causes endothelial dysfunction in children in the absence of OSAS. This study examines endothelial function in obese and non-obese children without OSAS.
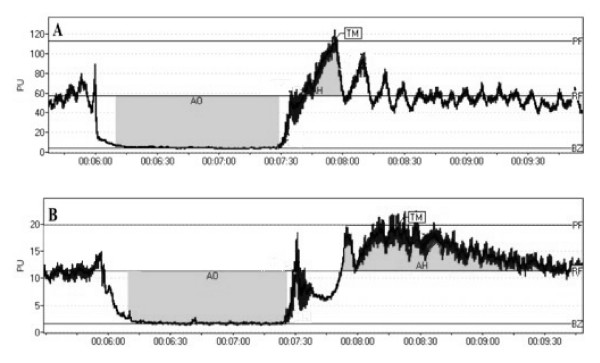
Methods: Pre-pubertal non-hypertensive children were recruited. Endothelial function was assessed in a morning fasted state, using a modified hyperemic test involving cuff-induced occlusion of the radial and ulnar arteries. The absence of OSAS was confirmed by overnight polysomnography. Anthropometry was also performed.
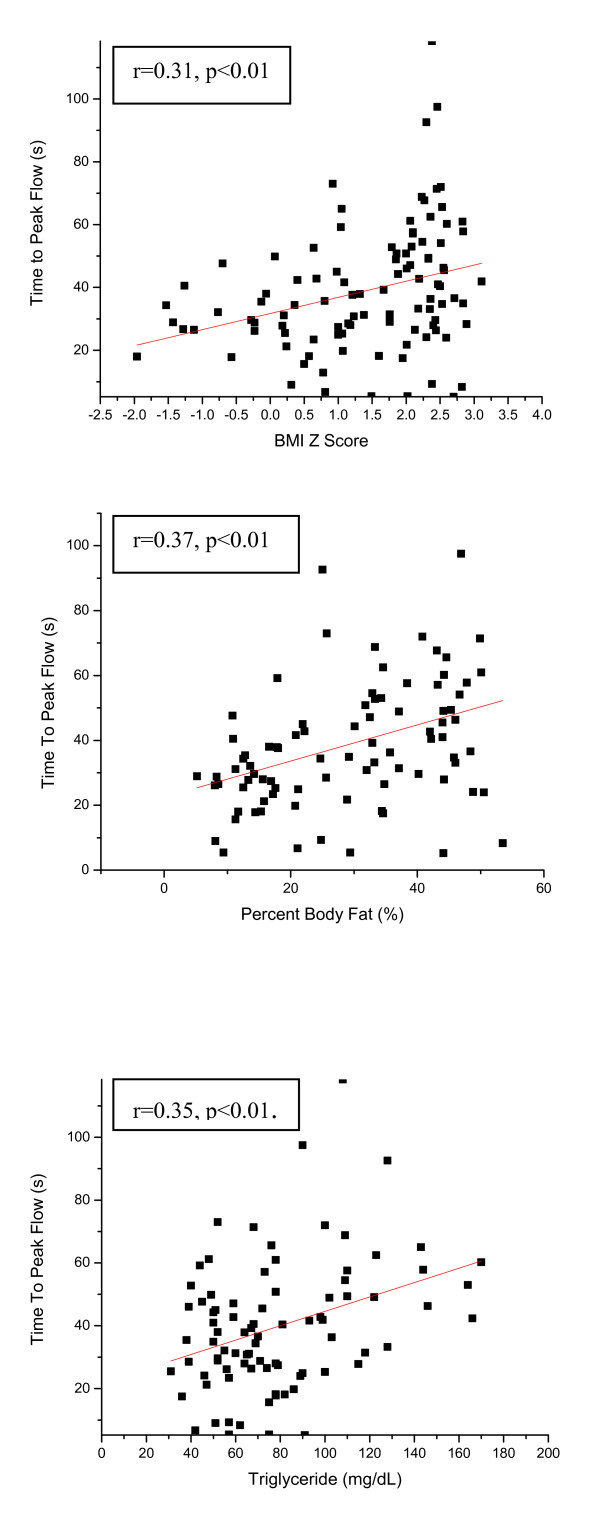
Results: 55 obese children (mean age 8.6 +/- 1.4 years, mean BMI z-score: 2.3 +/- 0.3) were compared to 50 non-obese children (mean age 8.0 +/- 1.6 years, mean BMI z-score 0.3 +/- 0.9). Significant delays to peak capillary reperfusion after occlusion release occurred in obese compared to non-obese children (45.3 +/- 21.9 sec vs. 31.5 +/- 14.1 sec, p < 0.01), but no differences in the magnitude of hyperemia emerged. Time to peak reperfusion and percentage of body fat were positively correlated (r = 0.365, p < 0.01).
Conclusions: Our findings confirm that endothelial dysfunction occurs early in life in obese children, even in the absence of OSAS. Thus, mechanisms underlying endothelial dysfunction in pediatric obesity are operational in the absence of sleep-disordered breathing.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
