

Surgically placed left ventricular leads provide similar outcomes to percutaneous leads in patients with failed coronary sinus lead placement
- PMID: 20156615
- PMCID: PMC3047450
- DOI: 10.1016/j.hrthm.2010.01.014
Surgically placed left ventricular leads provide similar outcomes to percutaneous leads in patients with failed coronary sinus lead placement
Abstract
Background: Cardiac resynchronization therapy using a left ventricular (LV) lead inserted via the coronary sinus (CS) improves symptoms of congestive heart failure, decreases hospitalizations, and improves survival. An epicardial LV lead is often placed surgically after a failed percutaneous attempt, but whether it offers the same benefits is unknown.
Objective: The purpose of this study was to determine if patients who receive a surgical LV lead after failed CS lead placement for cardiac resynchronization therapy derive the same benefit as do patients with a successfully placed CS lead.
Methods: A total of 452 patients underwent attempted CS lead insertion. Forty-five patients who had failed CS lead placement and then had surgical LV lead placement were matched with 135 patients who had successful CS lead placement.
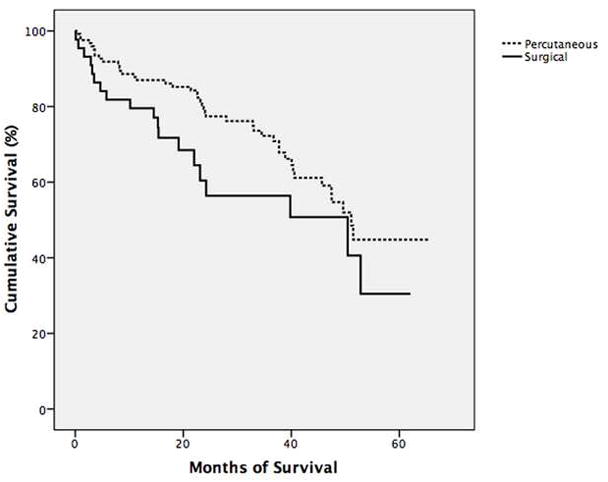
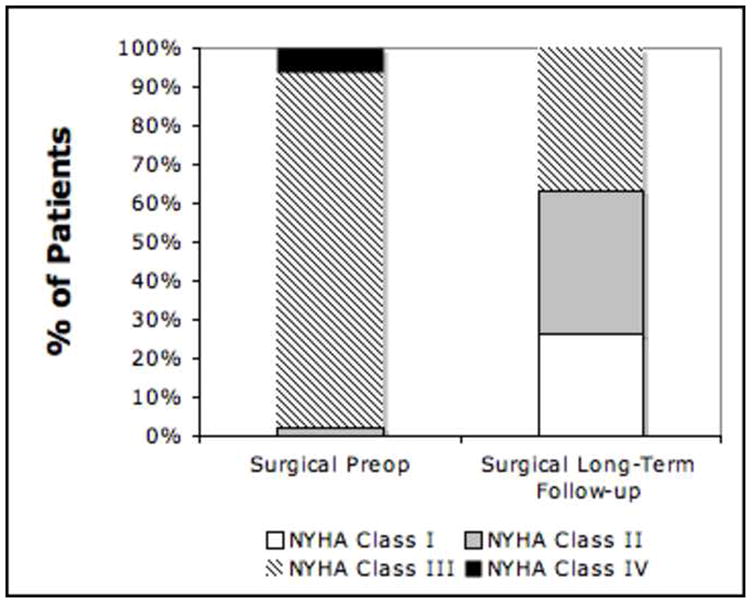
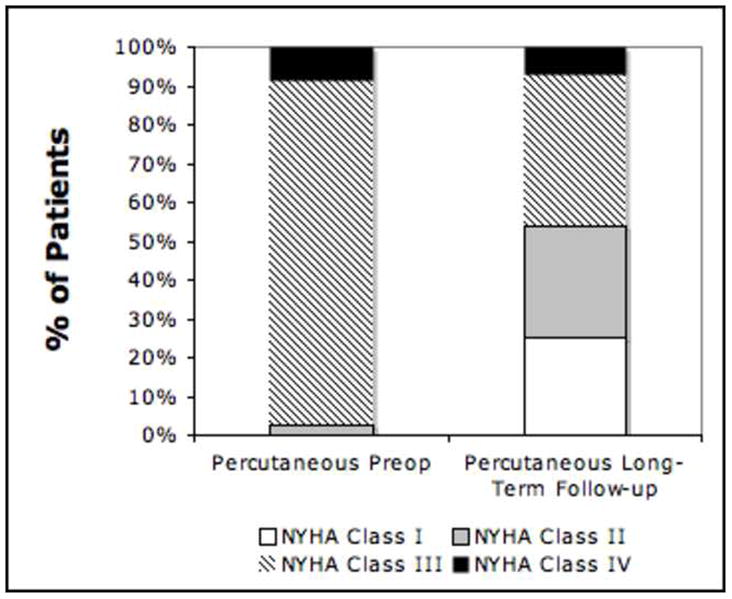
Results: No major differences in preoperative variables were seen between groups. Postprocedural complications of acute renal injury (26.2% vs 4.9%, P <.001) and infection (11.9% vs 2.4%, P = .03) were more common in the surgical group. Mean long-term follow-up was 32.4 +/- 17.5 months for surgical patients and 39.4 +/- 14.8 months for percutaneous patients. At follow-up, all-cause mortality (30.6% vs 23.8%, P = .22) and readmission for congestive heart failure (26.2% vs 31.5%, P = .53) were similar between surgical and percutaneous groups. Improvement in New York Heart Association functional class (60.1% vs 49.6%, P = .17) was similar between surgical and percutaneous groups.
Conclusion: Surgical LV lead placement offers functional benefits similar to those of percutaneous placement but with greater risk of perioperative complications, including acute renal failure and infection.
Copyright 2010 Heart Rhythm Society. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflicts of Interest: None
Figures
Similar articles
-
Surgical epicardial left ventricular lead versus coronary sinus lead placement in biventricular pacing.Eur J Cardiothorac Surg. 2005 Feb;27(2):235-42. doi: 10.1016/j.ejcts.2004.09.029. Eur J Cardiothorac Surg. 2005. PMID: 15691676
-
Reverse ventricular remodeling and long-term survival in patients undergoing cardiac resynchronization with surgically versus percutaneously placed left ventricular pacing leads.Heart Rhythm. 2015 Mar;12(3):517-523. doi: 10.1016/j.hrthm.2014.11.013. Epub 2014 Nov 13. Heart Rhythm. 2015. PMID: 25460866
-
Epicardial left ventricular lead placement for cardiac resynchronization therapy following failed coronary sinus approach.Congest Heart Fail. 2006 Nov-Dec;12(6):312-6. doi: 10.1111/j.1527-5299.2006.05568.x. Congest Heart Fail. 2006. PMID: 17170584
-
Percutaneous coronary sinus interventions to facilitate implantation of left ventricular lead: a case series and review of literature.J Card Fail. 2012 Apr;18(4):321-9. doi: 10.1016/j.cardfail.2012.01.003. J Card Fail. 2012. PMID: 22464774 Review.
-
Alternative techniques for left ventricular pacing in cardiac resynchronization therapy.Pacing Clin Electrophysiol. 2014 Feb;37(2):255-61. doi: 10.1111/pace.12320. Epub 2013 Dec 6. Pacing Clin Electrophysiol. 2014. PMID: 24313269 Review.
Cited by
-
Navigating Challenging Left Ventricular Lead Placements for Cardiac Resynchronization Therapy.J Innov Card Rhythm Manag. 2020 May 15;11(5):4107-4117. doi: 10.19102/icrm.2020.110505. eCollection 2020 May. J Innov Card Rhythm Manag. 2020. PMID: 32461816 Free PMC article. Review.
-
His-bundle pacing in a patient with dextrocardia, severe systolic dysfunction, and complete atrioventricular block.HeartRhythm Case Rep. 2018 Nov 30;5(3):148-151. doi: 10.1016/j.hrcr.2018.11.016. eCollection 2019 Mar. HeartRhythm Case Rep. 2018. PMID: 30891412 Free PMC article. No abstract available.
-
Event-free survival following CRT with surgically implanted LV leads versus standard transvenous approach.Pacing Clin Electrophysiol. 2011 Apr;34(4):490-500. doi: 10.1111/j.1540-8159.2010.03014.x. Pacing Clin Electrophysiol. 2011. PMID: 21463344 Free PMC article.
-
Cardiac Implantable Electronic Devices in Hemodialysis and Chronic Kidney Disease Patients-An Experience-Based Narrative Review.J Clin Med. 2021 Apr 17;10(8):1745. doi: 10.3390/jcm10081745. J Clin Med. 2021. PMID: 33920553 Free PMC article. Review.
-
Non-traditional implantable cardioverter-defibrillator configurations and insertion techniques: a review of contemporary options.Europace. 2022 Feb 2;24(2):181-192. doi: 10.1093/europace/euab178. Europace. 2022. PMID: 34453529 Free PMC article. Review.
References
-
- Abraham WT, Fisher WG, Smith AL, Delurgio DB, Leon AR, Loh E, Kocovic DZ, Packer M, Clavell AL, Hayes DL, Ellestad M, Trupp RJ, Underwood J, Pickering F, Truex C, McAtee P, Messenger J. Cardiac resynchronization in chronic heart failure. The New England journal of medicine. 2002;346(24):1845–1853. - PubMed
-
- Cesario DA, Turner JW, Dec GW. Biventricular pacing and defibrillator use in chronic heart failure. Cardiology clinics. 2007;25(4):595–603. vii. - PubMed
-
- Frattini F, Rordorf R, Angoli L, Pentimalli F, Vicentini A, Petracci B, Magrini G, Landolina M. Left ventricular pacing lead positioning in the target vein of the coronary sinus: description of a challenging case. Pacing Clin Electrophysiol. 2008;31(4):503–505. - PubMed
-
- Mair H, Jansens JL, Lattouf OM, Reichart B, Dabritz S. Epicardial lead implantation techniques for biventricular pacing via left lateral mini-thoracotomy, video-assisted thoracoscopy, and robotic approach. The heart surgery forum. 2003;6(5):412–417. - PubMed
-
- Yeim S, Bordachar P, Reuter S, Laborderie J, O’Neill MD, Lafitte S, Deplagne A, Garrigue S, Roudaut R, Jais P, Haissaguerre M, Dossantos P, Clementy J. Predictors of a positive response to biventricular pacing in patients with severe heart failure and ventricular conduction delay. Pacing Clin Electrophysiol. 2007;30(8):970–975. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
