A case of acquired Brown syndrome after surgical repair of a medial orbital wall fracture
- PMID: 20157416
- PMCID: PMC2817826
- DOI: 10.3341/kjo.2010.24.1.53
A case of acquired Brown syndrome after surgical repair of a medial orbital wall fracture
Abstract
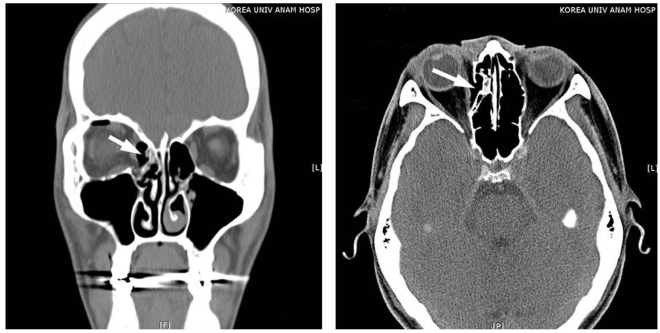
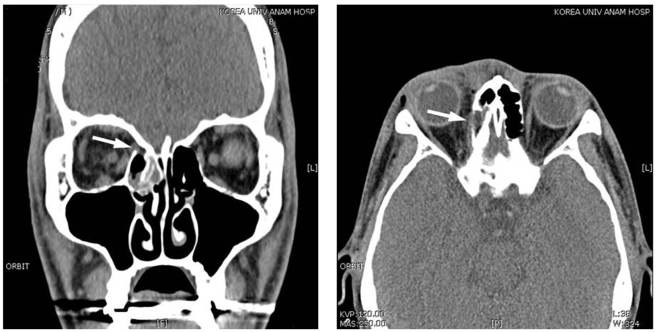
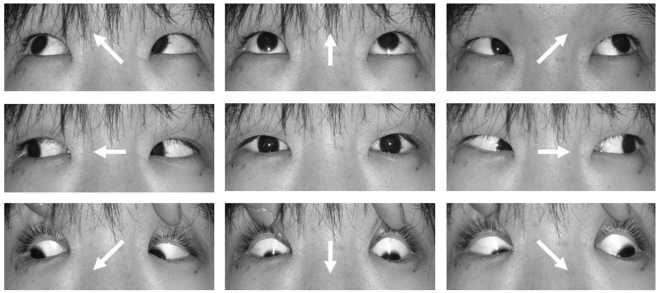
A case of acquired Brown syndrome caused by surgical repair of medial orbital wall fracture is reported in the present paper. A 23-year-old man presented at the hospital with right periorbital trauma. Although the patient did not complain of any diplopia, the imaging study revealed a blow-out fracture of the medial orbital wall. Surgical repair with a calvarial bone autograft was performed at the department of plastic surgery. The patient was referred to the ophthalmologic department due to diplopia that newly developed after surgery. The prism cover test at distant fixation showed hypotropia of the right eye, which was 4 prism diopters (PD) in primary gaze, 20 PD in left gaze, while orthophoric in right gaze. Eye movement of the right eye was markedly limited on elevation in adduction with normal elevation in abduction with intorsion in the right eye present. Forced duction test of the right eye showed restricted elevation in adduction. Computerized tomography scan of the orbits showed the right superior oblique muscle was entrapped between the autografted bone fragment and posterior margin of the fracture. When repairing medial orbital wall fracture that causes Brown syndrome, surgeons should always be careful of entrapment of the superior oblique muscle if the implant is inserted without identifying the superior and posterior margin of the orbital fracture site.
Keywords: Acquired Brown syndrome; Blow-out fracture; Ocular motility disorders; Orbital fractures; Superior oblique muscle entrapment.
Figures
Similar articles
-
Acquired simulated brown syndrome following surgical repair of medial orbital wall fracture.Korean J Ophthalmol. 2005 Mar;19(1):80-3. doi: 10.3341/kjo.2005.19.1.80. Korean J Ophthalmol. 2005. PMID: 15929493
-
Pseudo-Brown syndrome: a potential ophthalmologic sequela after a transcaruncular-transconjunctival approach for orbital fracture repair.J Oral Maxillofac Surg. 2012 Aug;70(8):1909-13. doi: 10.1016/j.joms.2012.03.015. Epub 2012 May 24. J Oral Maxillofac Surg. 2012. PMID: 22632930
-
Prospective study on ocular motility limitation due to orbital muscle entrapment or impingement associated with orbital wall fracture.Injury. 2017 Jul;48(7):1408-1416. doi: 10.1016/j.injury.2017.04.039. Epub 2017 Apr 21. Injury. 2017. PMID: 28499464
-
Superior oblique muscle entrapment in orbital fracture presenting as acquired brown-like syndrome: a case report and review of literature.Ophthalmic Plast Reconstr Surg. 2014 Mar-Apr;30(2):e26-8. doi: 10.1097/IOP.0b013e31829164b2. Ophthalmic Plast Reconstr Surg. 2014. PMID: 23719196 Review.
-
Navigating the Rare Medial Rectus Entrapment in Orbital Fractures: A 5-Year Series and Systematic Review of the Literature.Ann Plast Surg. 2025 May 1;94(5S Suppl 3):S446-S451. doi: 10.1097/SAP.0000000000004205. Ann Plast Surg. 2025. PMID: 40310008
Cited by
-
A Rare Case of Cyclotorsion Due to Medial Rectus Displacement Following Orbital Trauma.Br Ir Orthopt J. 2021 Apr 15;17(1):79-84. doi: 10.22599/bioj.165. eCollection 2021. Br Ir Orthopt J. 2021. PMID: 34278222 Free PMC article.
-
Brown syndrome with severe amblyopia: a case report from Africa.Pan Afr Med J. 2015 Jan 21;20:56. doi: 10.11604/pamj.2015.20.56.6050. eCollection 2015. Pan Afr Med J. 2015. PMID: 26090014 Free PMC article.
-
Three cases of acquired simulated brown syndrome after blowout fracture operations.Arch Plast Surg. 2015 May;42(3):346-50. doi: 10.5999/aps.2015.42.3.346. Epub 2015 May 14. Arch Plast Surg. 2015. PMID: 26015892 Free PMC article.
References
-
- Parks MM, Brown M. Superior oblique tendon sheath syndrome of Brown. Am J Ophthalmol. 1975;79:82–86. - PubMed
-
- von Noorden GK. Binocular vision and ocular motility: theory and management of strabismus. 3rd ed. St. Louis: Mosby; 1985. pp. 380–381.
-
- Ball SF, Ellis GS, Jr, Herrington RG, Liang K. Brown's superior oblique tendon syndrome after Baerveldt glaucoma implant. Arch Ophthalmol. 1992;110:1368–1369. - PubMed
-
- Muñoz M, Rosenbaum AL. Long-term strabismus complications following retinal detachment surgery. J Pediatr Ophthalmol Strabismus. 1987;24:309–314. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical