

The prosurvival activity of ascites against TRAIL is associated with a shorter disease-free interval in patients with ovarian cancer
- PMID: 20157422
- PMCID: PMC2821314
- DOI: 10.1186/1757-2215-3-1
The prosurvival activity of ascites against TRAIL is associated with a shorter disease-free interval in patients with ovarian cancer
Abstract
Background: The production of ascites is a common complication of ovarian cancer. Ascites constitute a unique tumor microenvironment that may affect disease progression. In this context, we recently showed that ovarian cancer ascites may protect tumor cells from TRAIL-induced apoptosis. In this study, we sought to determine whether the prosurvival effect of ascites affects disease-free intervals.
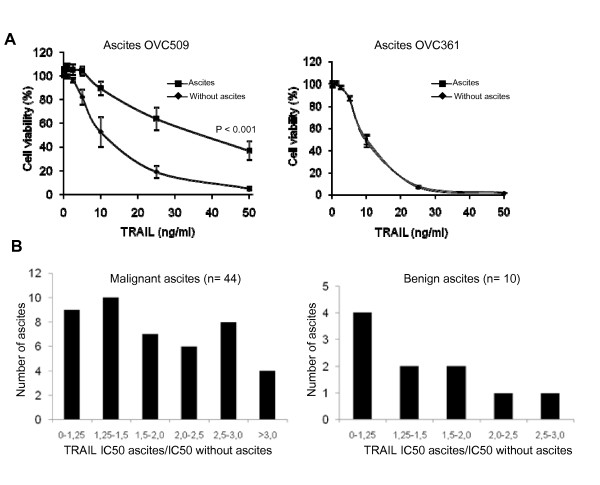
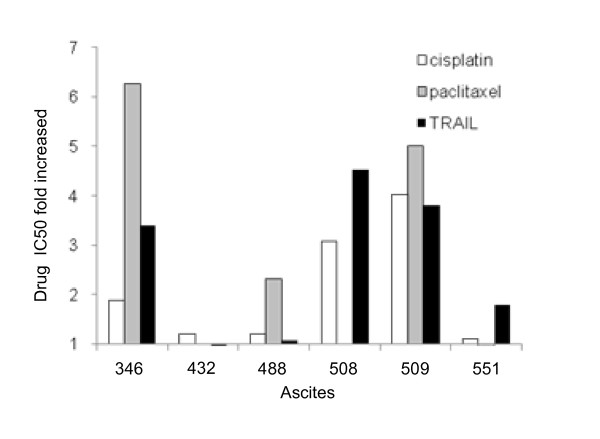
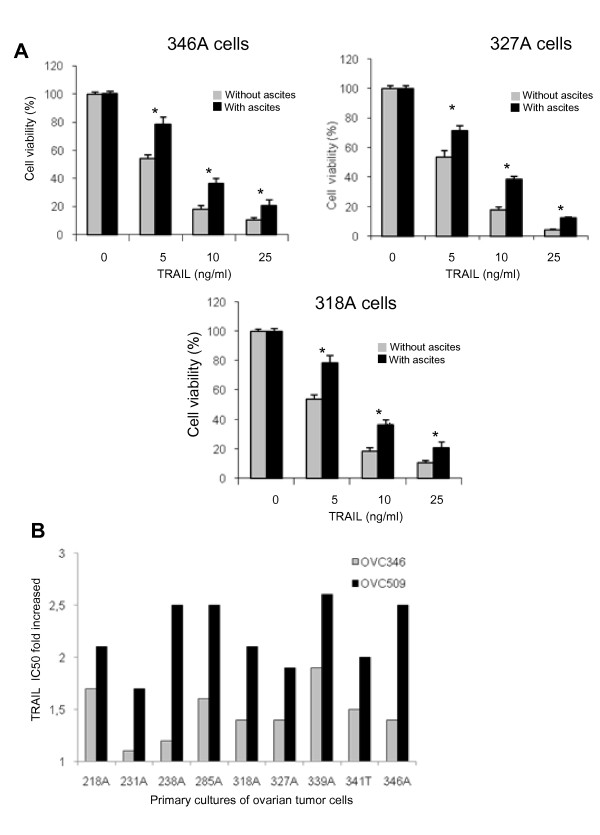
Methods: Peritoneal fluids were obtained from 54 women undergoing intra-abdominal surgery for suspected ovarian cancer (44 cancers and 10 benign diseases). The ability of peritoneal fluids to protect from TRAIL was assessed in the ovarian cancer cell line CaOV3, and IC(50 )were determined. The anti-apoptotic activity of 6 ascites against cisplatin, paclitaxel, doxorubicin, etoposide and vinorelbine was also assessed in CaOV3 cells, and the prosurvival activity of two ascites was assessed in 9 primary ovarian cancer cultures.
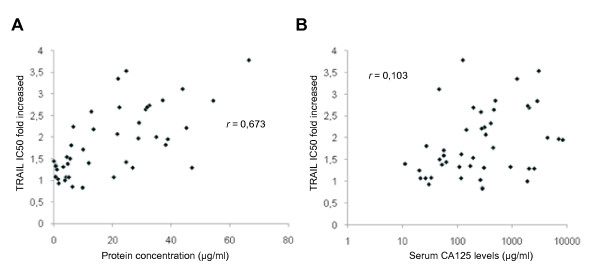
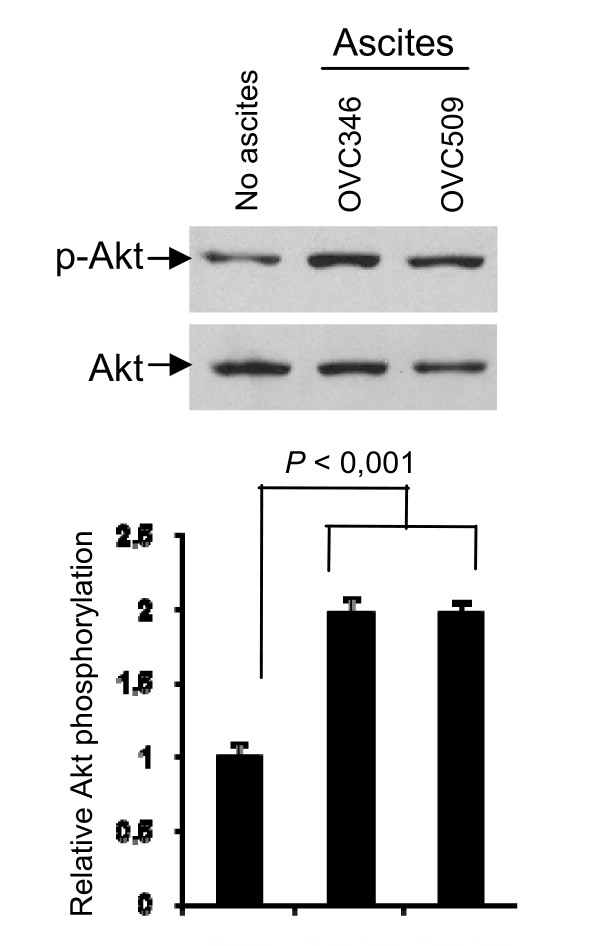
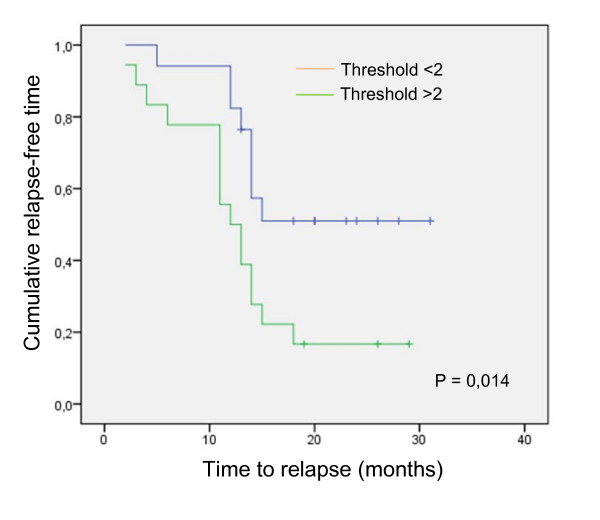
Results: Among the 54 peritoneal fluids tested, inhibition of TRAIL cytotoxicity was variable. Fluids originating from ovarian cancer were generally more protective than fluids from non-malignant diseases. Most of the 44 ovarian cancer ascites increased TRAIL IC(50 )and this inhibitory effect did not correlate strongly with the protein concentration in these ascites or the levels of serum CA125, a tumor antigen which is used in the clinic as a marker of tumor burden. The effect of ascites on cisplatin- and paclitaxel-induced cell death was assessed with 4 ascites having inhibitory effect on TRAIL-induced cell death and 2 that do not. The four ascites with prosurvival activity against TRAIL had some inhibitory on cisplatin and/or paclitaxel. Two ovarian cancer ascites, OVC346 and OVC509, also inhibited TRAIL cytotoxicity in 9 primary cultures of ovarian tumor and induced Akt activation in three of these primary cultures. Among a cohort of 35 patients with ascites, a threshold of TRAIL IC(50 )with ascites/IC(50 )without ascites > 2 was associated with shorter disease-free interval.
Conclusions: The prosurvival activity of ascites against TRAIL is associated with shorter disease-free interval, which may be explained, at least in part, by ascites-induced cisplatin/paclitaxel resistance. Our findings suggest that ascites may contain prosurvival factors that protect against TRAIL and chemotherapy and consequently affect disease progression.
Figures
References
-
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, Thun MJ. Cancer statistics, 2008. CA Cancer J Clin. 2008;49:8–31. - PubMed
-
- Mills GB, May C, McGill M, Roifman CM, Mellors A. A putative new growth factor in ascitic fluid from ovarian cancer patients: identification, characterization, and mechanism of action. Cancer Res. 1988;48:1066–1071. - PubMed
-
- Xu Y, Gaudette DC, Boynton JD, Frankel A, Fang XJ, Sharma A, Hurteau J, Casey G, Goodbody A, Mellors A, Holub BJ, Mills GB. Characterization of an ovarian cancer activating factor in ascites of ovarian cancer patients. Clin Cancer Res. 1995;1:1223–1232. - PubMed
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
Miscellaneous
