A contingency-management intervention to promote initial smoking cessation among opioid-maintained patients
- PMID: 20158293
- PMCID: PMC3605744
- DOI: 10.1037/a0018649
A contingency-management intervention to promote initial smoking cessation among opioid-maintained patients
Abstract
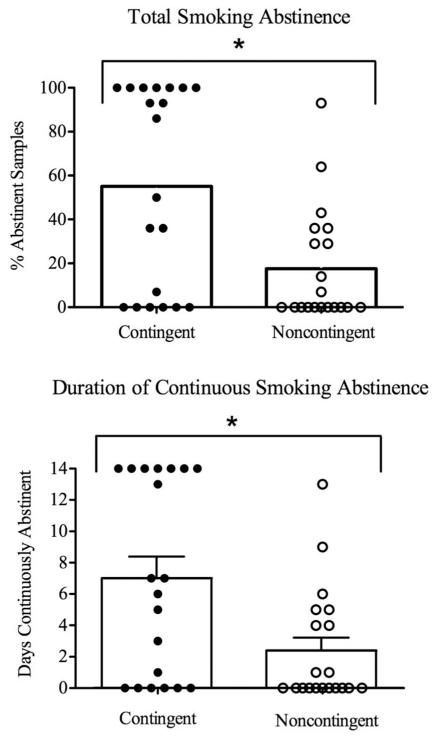
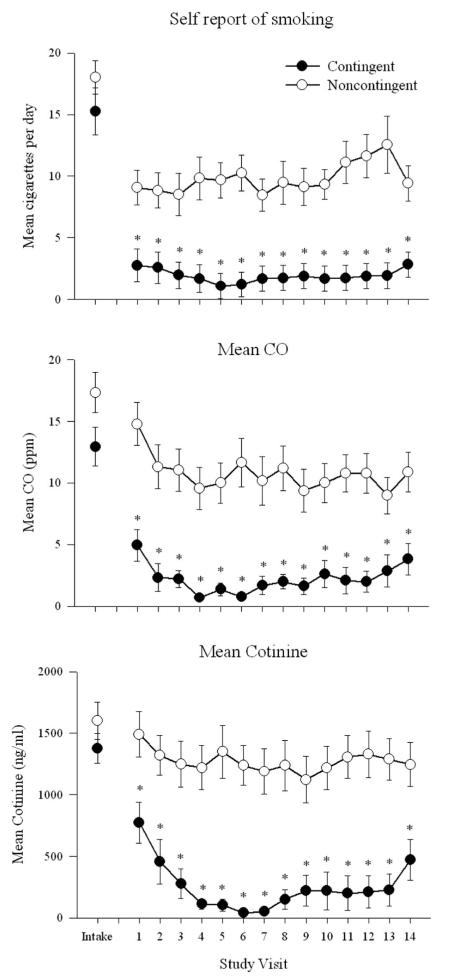
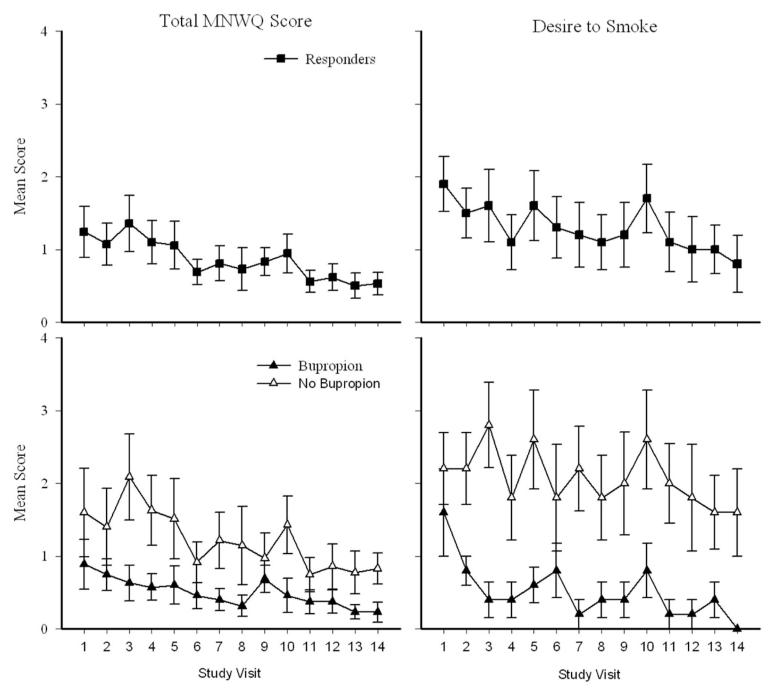
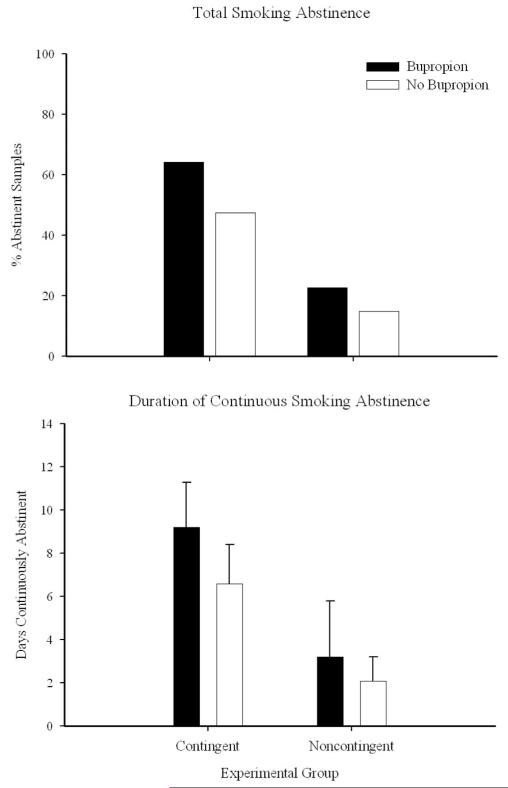
Prevalence of cigarette smoking among opioid-maintained patients is more than threefold that of the general population and associated with increased morbidity and mortality. Relatively few studies have evaluated smoking interventions in this population. The purpose of the present study was to examine the efficacy of contingency management for promoting initial smoking abstinence. Forty methadone- or buprenorphine-maintained cigarette smokers were randomly assigned to a contingent (n = 20) or noncontingent (n = 20) experimental group and visited the clinic for 14 consecutive days. Contingent participants received vouchers based on breath carbon monoxide levels during Study Days 1 to 5 and urinary cotinine levels during Days 6 to 14. Voucher earnings began at $9.00 and increased by $1.50 with each subsequent negative sample for maximum possible of $362.50. Noncontingent participants earned vouchers independent of smoking status. Although not a primary focus, participants who were interested and medically eligible could also receive bupropion (Zyban). Contingent participants achieved significantly more initial smoking abstinence, as evidenced by a greater percentage of smoking-negative samples (55% vs. 17%) and longer duration of continuous abstinence (7.7 vs. 2.4 days) during the 2 week quit attempt than noncontingent participants, respectively. Bupropion did not significantly influence abstinence outcomes. Results from this randomized clinical trial support the efficacy of contingency management interventions in promoting initial smoking abstinence in this challenging population.
(PsycINFO Database Record (c) 2010 APA, all rights reserved).
Figures
References
-
- Armitage P. Exclusions, losses to follow-up, and with-drawals in clinical trials. In: Shapiro SH, Lewis TA, editors. Clinical trials: Issues and approaches. Dekker; New York, NY: 1983. pp. 99–113.
-
- Beck AT, Beck RW. Screening depressed patients in family practice: A rapid technique. Postgraduate Medicine. 1972;52(6):81–85. - PubMed
-
- Bigelow GE, Stitzer ML, Griffiths RR, Liebson IA. Contingency management approaches to drug self-administration and drug abuse: Efficacy and limitations. Addictive Behaviors. 1981;6:241–252. - PubMed
-
- Centers for Disease Control Annual smoking-attributable mortality, years of potential life lost, and economic costs— United States, 1997-2001. Morbidity and Mortality Weekly Report. 2005;55:625–628. - PubMed
-
- Centers for Disease Control Use of cessation methods among smokers aged 16-24 years—United States 2003. Morbidity and Mortality Weekly Report. 2006;55:1351–1354. - PubMed