

Evidence in support of a role for anti-angiogenic factors in preterm prelabor rupture of membranes
- PMID: 20158393
- PMCID: PMC3104674
- DOI: 10.3109/14767050903440471
Evidence in support of a role for anti-angiogenic factors in preterm prelabor rupture of membranes
Abstract
Objective: Vaginal bleeding, placental abruption, and defective placentation are frequently observed in patients with preterm prelabor rupture of membranes (PROM). Recently, a role of vascular endothelial growth factor (VEGF) and its receptor, VEGF receptor (VEGFR)- 1 has been implicated in the mechanisms of membrane rupture. The purpose of this study was to determine whether the soluble form of VEGFR-1 and -2 concentrations in amniotic fluid (AF) change with preterm PROM, intra-amniotic infection/inflammation (IAI), or parturition.
Study design: This cross-sectional study included 544 patients in the following groups: (1) midtrimester (MT) (n = 48); (2) preterm labor (PTL) leading to term delivery (n = 143); (3) PTL resulting in preterm delivery with (n = 72) and without IAI (n = 100); (4) preterm PROM with (n = 46) and without IAI (n = 42); (5) term in labor (n = 48); and (6) term not in labor (n = 45). The concentrations of sVEGFR-1 and sVEGFR-2 were determined by ELISA. Non-parametric statistics and logistic regression analysis were applied.
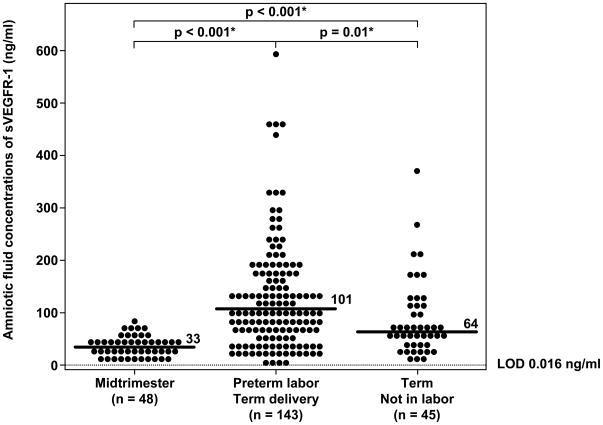
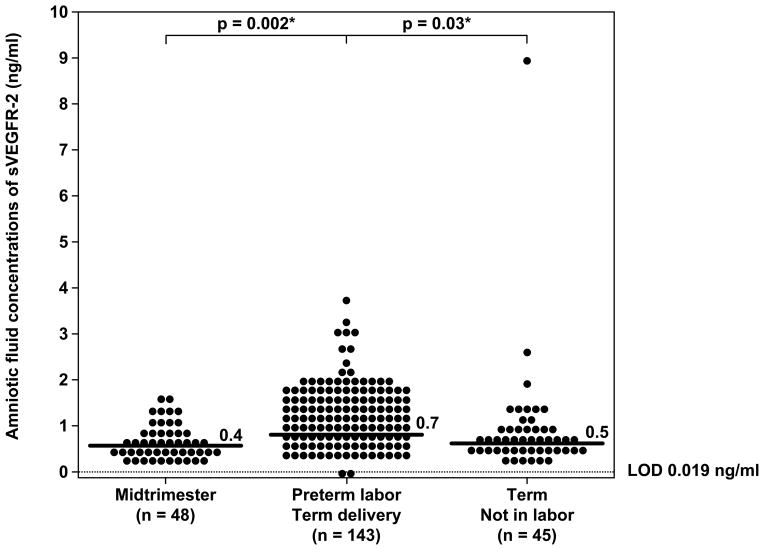
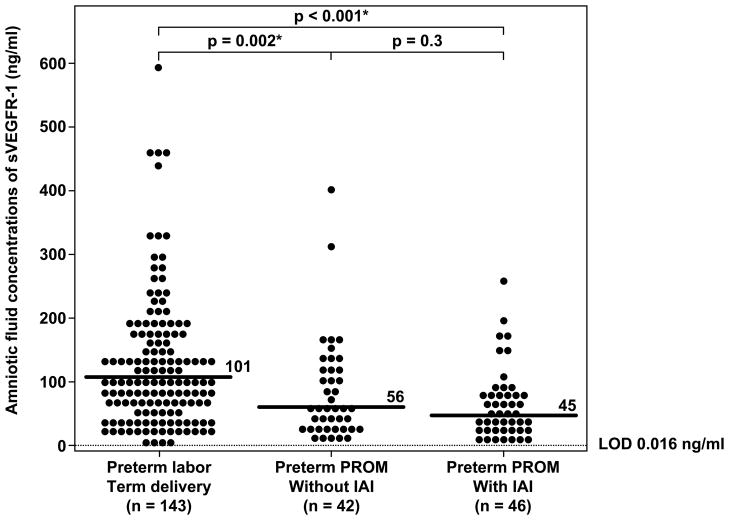
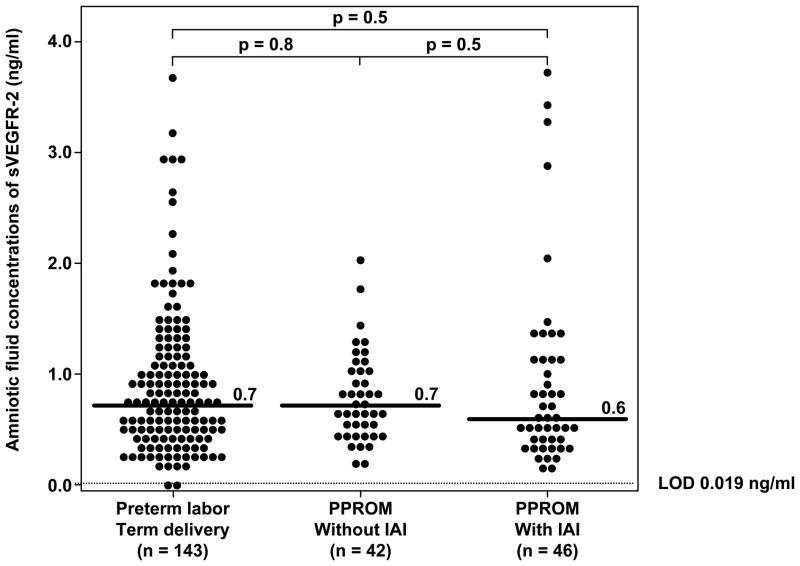
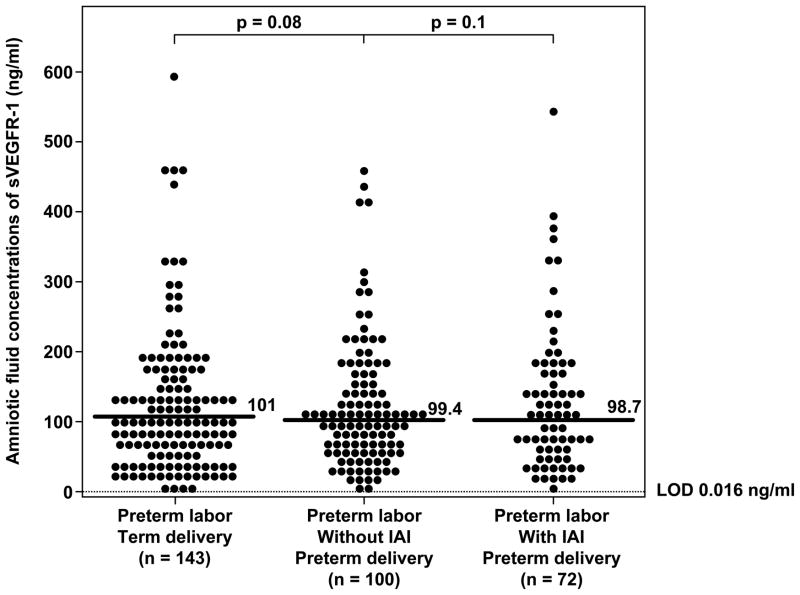
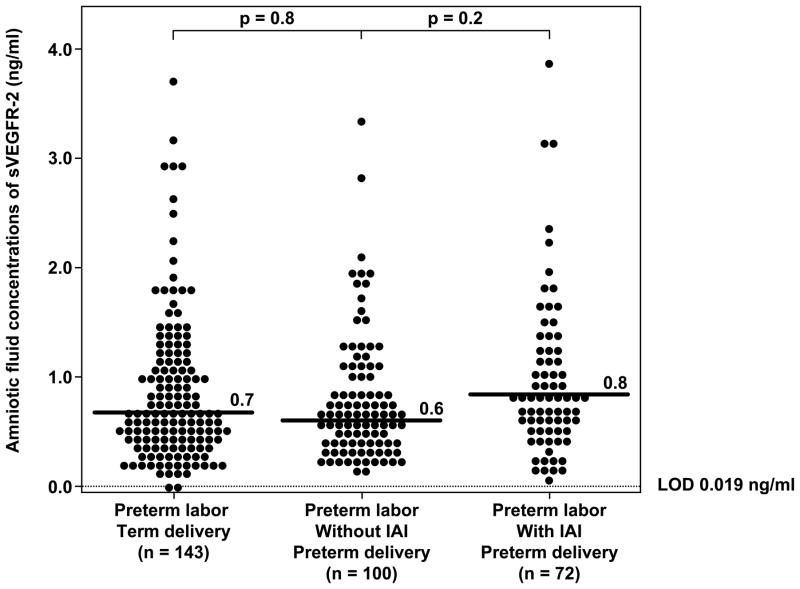
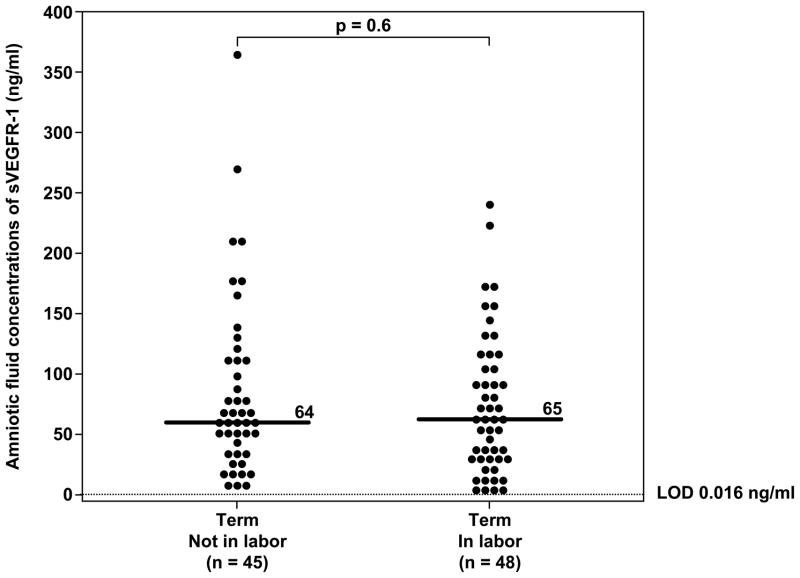
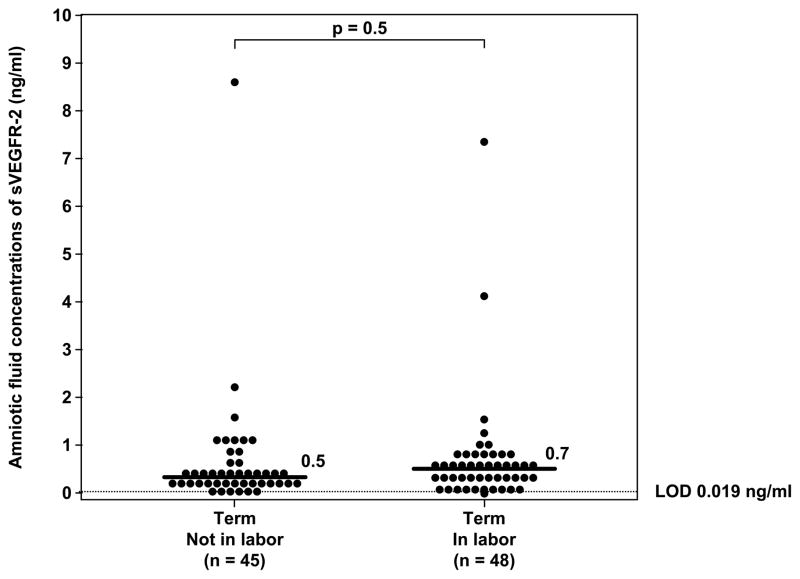
Results: (1) Preterm PROM (with and without IAI) had a lower median AF concentration of sVEGFR-1 than patients with PTL who delivered at term (p < 0.001 for each comparison); (2) A decrease in AFsVEGFR-1 concentrations per each quartile was associated with PROM after adjusting for confounders (OR 1.8; 95%CI 1.4-2.3); (3) IAI, regardless of the membrane status, was not associated with a change in the median AF concentrations of sVEGFR-1 and sVEGFR-2 (p > 0.05 for each comparison); and (4) Spontaneous term and PTL did not change the median sVEGFR-1 and sVEGFR-2 concentrations (p > 0.05 for each comparison).
Conclusion: (1) This is the first evidence that preterm PROM is associated with a lower AF concentration of sVEGFR-1 than patients with PTL intact membranes. These findings cannot be attributed to gestational age, labor, or IAI; and (2) AF concentrations of sVEGFR-2 did not change with preterm PROM, IAI, or labor at term and preterm.
Figures
References
-
- Santolaya-Forgas J, Romero R, Espinoza J, Erez O, Friel L, Kusanovic JP, Bahado-Singh R, Nien JK. 3. 2006. Prelabor rupture of the membranes; pp. 1130–1188.
-
- Gibbs RS, Blanco JD. Premature rupture of the membranes. Obstet Gynecol. 1982;60:671–679. - PubMed
-
- Parry S, Strauss JF., III Premature rupture of the fetal membranes. N Engl J Med. 1998;338:663–670. - PubMed
-
- Gunn GC, Mishell DR, Jr, Morton DG. Premature rupture of the fetal membranes. A review. Am J Obstet Gynecol. 1970;106:469–483. - PubMed
-
- Mercer BM. Preterm premature rupture of the membranes: current approaches to evaluation and management. Obstet Gynecol Clin North Am. 2005;32:411–428. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources