

Molecular imaging in thyroid cancer
- PMID: 20159663
- PMCID: PMC2842177
- DOI: 10.1102/1470-7330.2010.0002
Molecular imaging in thyroid cancer
Abstract
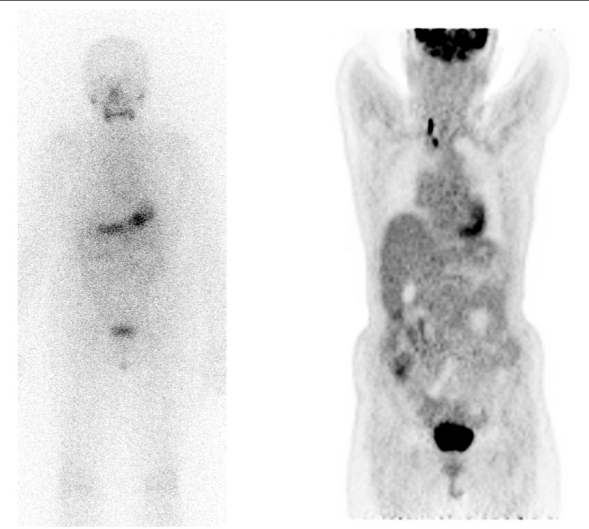
Molecular imaging plays an important role in the evaluation and management of thyroid cancer. The routine use of thyroid scanning in all thyroid nodules is no longer recommended by many authorities. In the initial work-up of a thyroid nodule, radioiodine imaging can be particularly helpful when the thyroid stimulating hormone level is low and an autonomously functioning nodule is suspected. Radioiodine imaging can also be helpful in the 10-15% of cases for which fine-needle aspiration biopsy is indeterminate. Therapy of confirmed thyroid cancer frequently involves administration of iodine-131 after surgery to ablate remnant tissue. In the follow-up of thyroid cancer patients, increased thyroglobulin levels will often prompt the empiric administration of 131I followed by whole body radioiodine imaging in the search for recurrent or metastatic disease. 131I imaging of the whole body and blood pharmacokinetics can be used to determine if higher doses of 131I can be given in thyroid cancer. The utility of [18F]fluorodeoxyglucose (FDG) positron emission tomography (PET) is steadily increasing. FDG is primarily taken up by dedifferentiated thyroid cancer cells, which are poorly iodine avid. Thus, it is particularly helpful in the patient with an increased thyroglobulin but negative radioiodine scan. FDG PET is also useful in the patient with a neck mass but unknown primary, in patients with aggressive (dedifferentiated) thyroid cancer, and in patients with differentiated cancer where histologic transformation to dedifferentiation is suspected. In rarer types of thyroid cancer, such as medullary thyroid cancer, FDG and other tracers such as 99mTc sestamibi, [11C]methionine, [111In]octreotide, and [68Ga]somatostatin receptor binding reagents have been utilized. 124I is not widely available, but has been used for PET imaging of thyroid cancer and will likely see broader applicability due to the advantages of PET methodology.
Figures
References
-
- American Cancer Society. Atlanta: American Cancer Society; 2009. Cancer facts & figures 2009. doi:10.2214/AJR.07.2848. PMid:18562736. - DOI
-
- Ron E. Thyroid cancer incidence among people living in areas contaminated by radiation from the Chernobyl accident. Health Phys. 2007;93:502–11. doi:10.1097/01.HP.0000279018.93081.29. PMid:18049226. - DOI - PubMed
-
- Naing S, Collins BJ, Schneider AB. Clinical behavior of radiation-induced thyroid cancer: factors related to recurrence. Thyroid. 2009;19:479–85. doi:10.1089/thy.2008.0343. PMid:19226197. - DOI - PMC - PubMed
-
- Seaberg RM, Eski S, Freeman JL. Influence of previous radiation exposure on pathologic features and clinical outcome in patients with thyroid cancer. Arch Otolaryngol Head Neck Surg. 2009;135:355–9. doi:10.1001/archoto.2009.13. PMid:19380356. - DOI - PubMed
-
- Ron E, Lubin JH, Shore RE, et al. Thyroid cancer after exposure to external radiation: a pooled analysis of seven studies. Radiat Res. 1995;141:259–77. doi:10.2307/3579003. PMid:7871153. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical