

Phase I clinical trial of the CYP17 inhibitor abiraterone acetate demonstrating clinical activity in patients with castration-resistant prostate cancer who received prior ketoconazole therapy
- PMID: 20159824
- PMCID: PMC2849769
- DOI: 10.1200/JCO.2009.24.1281
Phase I clinical trial of the CYP17 inhibitor abiraterone acetate demonstrating clinical activity in patients with castration-resistant prostate cancer who received prior ketoconazole therapy
Abstract
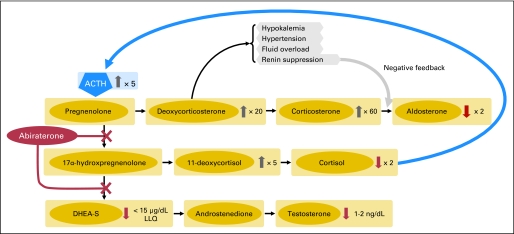
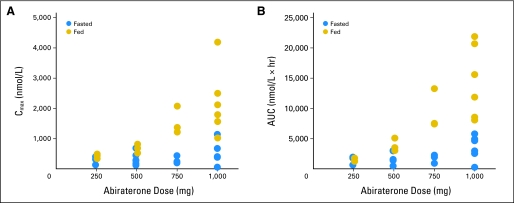
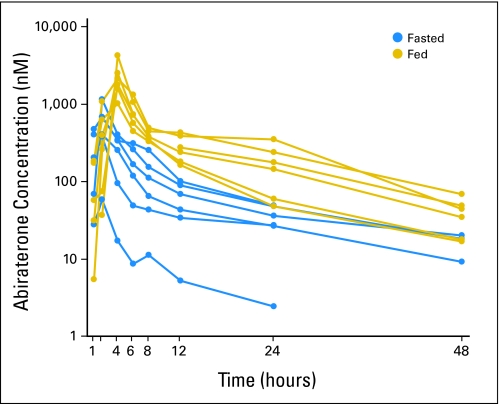
Purpose: Abiraterone acetate is a prodrug of abiraterone, a selective inhibitor of CYP17, the enzyme catalyst for two essential steps in androgen biosynthesis. In castration-resistant prostate cancers (CRPCs), extragonadal androgen sources may sustain tumor growth despite a castrate environment. This phase I dose-escalation study of abiraterone acetate evaluated safety, pharmacokinetics, and effects on steroidogenesis and prostate-specific antigen (PSA) levels in men with CPRC with or without prior ketoconazole therapy.
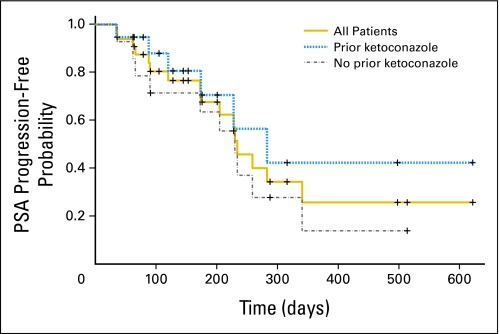
Patients and methods: Thirty-three men with chemotherapy-naïve progressive CRPC were enrolled. Nineteen patients (58%) had previously received ketoconazole for CRPC. Bone metastases were present in 70% of patients, and visceral involvement was present in 18%. Three patients (9%) had locally advanced disease without distant metastases. Fasted or fed cohorts received abiraterone acetate doses of 250, 500, 750, or 1,000 mg daily. Single-dose pharmacokinetic analyses were performed before continuous daily dosing.
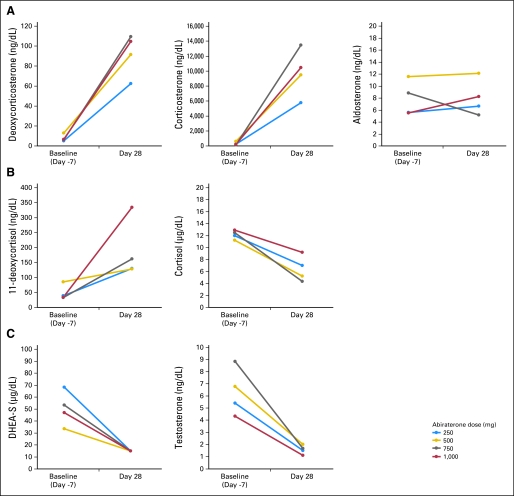
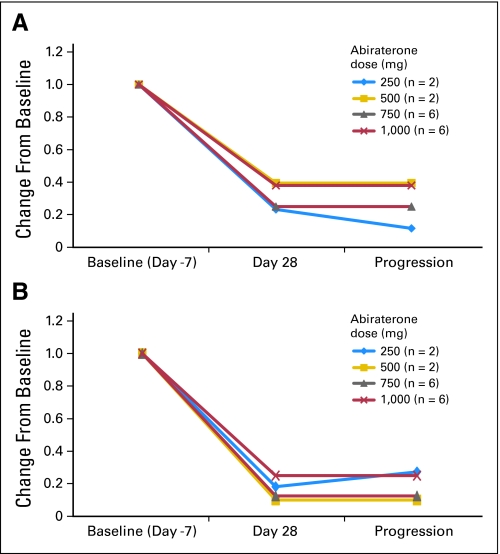
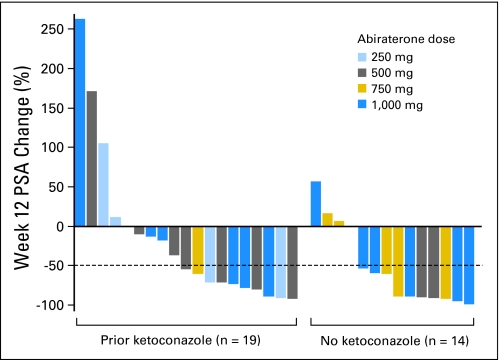
Results: Adverse events were predominantly grade 1 or 2. No dose-limiting toxicities were observed. Hypertension (grade 3, 12%) and hypokalemia (grade 3, 6%; grade 4, 3%) were the most frequent serious toxicities and responded to medical management. Confirmed > or = 50% PSA declines at week 12 were seen in 18 (55%) of 33 patients, including nine (47%) of 19 patients with prior ketoconazole therapy and nine (64%) of 14 patients without prior ketoconazole therapy. Substantial declines in circulating androgens and increases in mineralocorticoids were seen with all doses.
Conclusion: Abiraterone acetate was well tolerated and demonstrated activity in CRPC, including in patients previously treated with ketoconazole. Continued clinical study is warranted.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Castration-resistant prostate cancer--hormone therapy redux.J Clin Oncol. 2010 Mar 20;28(9):1447-9. doi: 10.1200/JCO.2009.25.3781. Epub 2010 Feb 16. J Clin Oncol. 2010. PMID: 20159817 No abstract available.
-
Abiraterone acetate is well tolerated without concomitant use of corticosteroids.J Clin Oncol. 2010 Oct 10;28(29):e560-1; author reply e562. doi: 10.1200/JCO.2010.29.5170. Epub 2010 Aug 30. J Clin Oncol. 2010. PMID: 20805462 No abstract available.
References
-
- Tannock IF, de Wit R, Berry WR, et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N Engl J Med. 2004;351:1502–1512. - PubMed
-
- Berthold DR, Pond GR, Soban F, et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer: Updated survival in the TAX 327 study. J Clin Oncol. 2008;26:242–245. - PubMed
-
- Petrylak DP, Tangen CM, Hussain MH, et al. Docetaxel and estramustine compared with mitoxantrone and prednisone for advanced refractory prostate cancer. N Engl J Med. 2004;351:1513–1520. - PubMed
-
- Slovin SF. Neuroendocrine differentiation in prostate cancer: A sheep in wolf's clothing? Nat Clin Pract Urol. 2006;3:138–144. - PubMed
-
- Pienta KJ, Bradley D. Mechanisms underlying the development of androgen-independent prostate cancer. Clin Cancer Res. 2006;12:1665–1671. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
